
A Comparative Study of Alexithymia and Social Anxiety in Infertile Men and Women
1Midwifery Department, College of Nursing , Shiraz University of Medical Sciences, Shiraz , Iran.
2Research Center for Social Determinants of Health, Jahrom University of Medical Sciences, Jahrom, Iran.
3Research committee, Jahrom University of Medical Sciences, Jahrom, Iran.
4Research and Clinical Center, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
5Research committee, Shiraz University of Medical Sciences, Shiraz , Iran.
Corresponding Author E-mail: Mosalanejad@jums.ac.ir
DOI : http://dx.doi.org/10.13005/bbra/2400
Download this article as:
![]()
Alexithymia and social anxiety are psychological disorders that can accompany infertility. Alexithymia is the inability to process, analyze, and regulate one's emotion, and social anxiety is the extreme fear of being scorned in social and practical situations.The objective of this study is to compare alexithymia and social anxiety in infertile men and women who visited the Infertility Center of Yazd, Iran. This is a cross-sectional descriptive study of 198 infertile couples who visited the Infertility Center of Yazd, Iran. The subjects were chosen on a convenience sampling method basis. The measuring instruments consisted of the Toronto Alexithymia Scale (TAS), a social anxiety inventory, and a demographics questionnaire. The collected data were analyzed using SPSS, descriptive statistics, Pearson correlation coefficient, and regression analysis. The results show that there is not a significant difference between the means alexithymia scores of the male and female groups. However, the overall level of alexithymia is higher in women than in men (59.50(11.88) versus 59.31(10.84), p=0.90). While men had a higher level of concrete thinking disorders, women had more problems with describing and expressing their emotions. The results also show that there is not a significant difference between the means of the two groups' scores in the subcategories of social anxiety. However, the men's mean score is higher in the subcategory of avoidance (6.87(3.96) vs 6.73(4.14)), and the women have higher scores in the other two subcategories of fear (7.90(4.44) vs 7.15(4.34)) and physiology (5.90(3.88) vs 5.52 (4.38). In view of the various psychological issues that can affect infertile men and women and subsequently lead to physical, emotional, and behavioral disorders, recognizing the problems of infertility can be helpful to health policy makers in developing effective educational programs
KEYWORDS:alexithymia; social anxiety; couples; infertility
Introduction
Infertility is a complicated issue that is defined as the failure to become pregnant after one year of having unprotected sex(1)). Infertility is a serious personal and social problem that can be accompanied by a variety of psychological disorders. While psychological factors can play a role in causing infertility, infertility itself can be the cause of a wide range of psychological disorders. Studies of the negative psychological, behavioral, and social consequences of infertility for both members of a couple show that infertile couples tend to experience a wide range of negative emotions, including anxiety, fear, avoidance, depression, guilt, and frustration(2-4) Other examples of psychological disorders that can accompany infertility are alexithymia and social anxiety. Alexithymia is the inability to process, analyze, and regulate one’s emotions (5). Alexithymia has three main characteristics: difficulty identifying emotions, difficulty describing emotions, and externally oriented cognitive style (6, 7). Difficulty identifying emotions happens when an individual is confused and unable to distinguish between emotions. Difficulty describing emotions refers to an individual’s inability to express what he/she has emotionally experienced. Externally oriented cognitive style is an individual’s tendency to contemplate matters externally, as opposed to an internally oriented cognitive style (8, 9).
Alexithymic individuals tend to exaggerate normal physical sensations and misinterpret the physical signs of emotional arousal. It is believed that alexithymia is a contributory factor in many psychological disorders. The construct of alexithymia indicates a cluster of cognitive and affective characteristics, including difficulties in recognizing and verbalizing feelings, in reaction to external events (10). On the other hand, infertile individuals’ failure to express and describe their emotions can result in their experiencing social anxiety or social phobia. Social phobia is an extreme fear of being scorned in social and practical situations, and is often characterized by an individual’s avoidance of such situations ((11).Social phobia is the fourth most prevalent psychological disorder in the United States; it is estimated that 12.1% of people are affected by it in their lifetime (12). Ellis and Hudson state that distress plays an important role in anxiety-related disorders, including generalized anxiety disorder and social anxiety (13). In Seibel’s study, the total prevalence of psychological problems in infertile couples is reported to be between 25% and 60% (3). In another study, 74.6% of the infertile individuals interviewed reported a change in their behavior (14).The psychological problems that affect infertile patients are complicated and influenced by a variety of factors, including gender, and cause and length of infertility. In view of the psychological consequences of infertility, the increase in concern over the psychological disorders caused by infertility is understandable. It is evident that infertility is a profoundly stressful experience for most couples (15). Some evidence reported that infertile women showed significantly higher rates of alexithymia than fertile women(16), and others found a significantly higher alexithymia rate in infertile men compared with fertile men. However, none of these studies compares the symptoms in couples, and there is no other research about this issue (6, 17).
Fertility is of utmost importance, both culturally and socially, to couples, especially women. Therefore, it is important that the probable psychological and social consequences of infertility be studied in depth.
The above-mentioned factors stress the need for greater attention to the psychological problems that can accompany infertility and taking steps toward dealing with these problems, alongside medical interventions. Considering the personal, social, and cultural significances of fertility and infertility, and the increasing prevalence of infertility and related psychological issues, studying the psychological aspects of infertility is essential. Accordingly, the present study aims to explore the prevalence of alexithymia and social anxiety, two of the psychological disorders that can affect infertile individuals, in infertile couples. Few studies in the world and no studies in Iran have addressed the incidence of the above-mentioned disorders in infertile couples. Some research has addressed the symptoms of these disorders in men or women alone, but there is no significant research to compare these symptoms in infertile couples.
Considering the special features of infertility in the Iranian culture, a study of these disorders in Iran can prove very beneficial.
The role of the infertility nurse and midwife is to provide a holistic approach to infertility investigation, treatment, and pregnancy through compassionate, informed, and evidence-based practice. This role allows for more personalized interactions with infertile patients, which provides new opportunities for infertility research. These caregivers work as part of multi-professional teams whose focus is on delivering a high standard of care. In order to increase the knowledge and scientific level of nurses and midwives in assistant reproductive therapy clinics, which will allow for better treatment for infertile patients, skillful counseling, promotion of collaboration with other members of the health care team on research and treatment, and incorporating appropriate and successful medical interventions should be prioritized. The aim of this study is to investigate alexithymia and social phobia in infertile couples and compare these disorders by gender difference.
Materials and Methods
This project is a cross-sectional study of 198 infertile couples who visited the Infertility Center of Yazd, Iran. The subjects were selected based on the convenience sampling method, using the following formula:
n = (z2–σ2) / d2
Where n = number of participant, z =, σ=, and d=2. With a significance value of 0.05, a required sample size of 102 was calculated.
Alfa=0.05 M+_SD:60.06 +_ 10.28 d=2 n=102
Participants
The population consisted of all infertile couples who visited the Infertility Center of Yazd, and the inclusion criteria were being Iranian and speaking Farsi. The exclusion criteria were suffering from a debilitating physical or mental illness and taking libido-reducing medication, such as antihypertensives, digoxin, and antidepressants. Before completing the questionnaires, the couples were informed of the objectives of the study and the proper manner of answering the questions. The participants were also assured that they were free to withdraw from the study at any point. The questionnaire was filled out by participants in at the first referral before any medical interventions, and the appropriate explanations were given by the researcher on how to complete the questionnaire. All questionnaires were completed by the participants and delivered to the same place. The data collection involved a two-part questionnaire: part one addressed the participants’ demographics (age, gender, field of study, education, length of marriage, length of infertility, and cause of infertility); part two included the Toronto Alexithymia Scale (TAS-20) and a social anxiety disorder inventory.
Data gathering
The TAS-20 is a 20-item questionnaire that assesses the three subscales of difficulty identifying emotions (7 items), difficulty describing emotions (5 items), and concrete thinking (8 items); scoring is based on a 5-point Likert scale, ranging from completely disagree (1 point) to completely agree (5 points). Composed of 17 items, the measure of social anxiety disorder addresses the topics of fear, avoidance, and physiological symptoms; the scores for each item can range between 0 and 4.
Many studies have analyzed the psychometric features of the TAS-20: the test-retest reliability of the scale was verified by a study with a sample of 67 individuals in two phases with a 4-week interval; the value of r was found to range between 0.80 and 0.87 for total alexithymia and its subscales. The concurrent validity of the TAS-20 has been verified based on correlation among the subscales of the test (5). Turner et al. used the test-retest method for the social anxiety inventory with a 2-week interval and found the reliability coefficient to be 0.86. This test normalized for Iranian people (18).
The Social Phobia Inventory, described by Connor et al.(1), consists of 17 items evaluated on a 5-point Likert scale (0–4) with a maximum total score of 68. This is purported to assess the spectrum of social anxiety disorder symptomatology. The psychometric qualities of this test were satisfactory, as shown by the following properties: test-retest reliability (0.78 to 0.89, p < 0.0001); internal consistency (Cronbach alpha) ranging from 0.68 to 0.94 for cases and from 0.57 to 0.90 for non-cases; sensitivity of 0.72 and specificity of 0.84 for the 19 cut-off point. This questionnaire was normalized for Iranian peoples (19).
 |
Figure 1: Alexithymia in male and female by infertility causes
|
Analysis
Analysis of descriptive statistics is presented as mean and SD, and analytic statistics were analyzed by student’s t-test for comparing the mean score of variables in two groups. The collected data were analyzed using SPSS (v 16).
Results
Externally-oriented thinking was higher in men (23.19%) than in women (22.02%), while the levels of the other two subscales–difficulty describing feelings and difficulty identifying feelings–were higher in women than in men (22.85 vs 21.68 and 14.65 vs 14.44, respectively).
Table 1 shows that there is a significant difference between men and women in the subscale of critical thinking, and this index is higher in men than in women. While the mean of women’s scores is higher than men’s for the difficulty describing emotion and difficulty identifying emotions indexes, the differences are not statistically significant. A comparison between the two groups’ alexithymia scores based on the point of cross section shows that, though the total degree of alexithymia is higher in women than in men, there are no significant differences between the two.
Table 1: Mean score of alexithymia in the two groups
| Alexithymia index | Group | mean±SD | P | 95% Confidence Interval of the Difference | |
| Lower | Upper | ||||
| Critical thinking | Female
Male |
22.01± 3.69
23.19 ± 2.92 |
.013 | -2.12760
-2.10352 |
-.22240
-.24648 |
| Identifying emotion | Female
Male |
22.84 ± 21.6
6.54 ± 6.31 |
.208 | -.65488
-.64802 |
2.98215
2.97530 |
| Describing
emotion |
Female
Male |
14.64 ±14.4
4.22 ± 3.85 |
.726 | -.94501
-.93341 |
1.34956
1.33796 |
| Toal alexithymia | Female
Male |
59.50 ±11.8
59.31 ±10.84 |
0.90 | -3.03
-3 |
3.41
3.38 |
Other results show that, when the cause of infertility is unknown, the frequency of the subscales of alexithymia is higher for both genders. (Figure1)
The frequency of alexithymia is highest when the length of infertility is between 10 to 15 years.
Table 2 shows that there are no significant differences between the groups in terms of the means of social anxiety subscales. However, the men have a higher mean score in avoidance, while the means of the women’s scores are higher in the other two subscales, fear and physiological symptoms.
Table 2: Mean score of social phobia in the two groups
| Social phobia | Groups | n | mean±SD | P | |
| phobia | female
male |
110
88 |
7.90 ± 7.15
4.44 ± 4.34 |
0.23 | |
| avoidant | female
male |
110
88 |
6.73 ± 6.87
4.14 ± 3.96 |
0.81 | |
| physiology | female
male |
110
88 |
5.90 ± 5.52
3.88 ± 4.38 |
0.52 | |
Figure 2 shows that the highest percentages of the subscales of social anxiety belong to women when the causes of infertility are mixed and when women themselves are responsible for infertility. The results also show that the level of social anxiety is highest when the length of infertility is greater than 10–15 years.
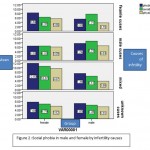 |
Figure 2: Social phobia in male and female by infertility causes
|
Discussion
The results showed that the subscale of externally-oriented thinking (EOT) is more prevalent in men than in women, while the other two subscales of alexithymia–difficulty describing feeling (DDF) and difficulty identifying feeling (DIF)–affect women more than men. The men’s mean score in EOT subscale was significantly higher than the women’s. However, though the women’s mean scores in DDF and DIF were higher than men’s, the differences were not statistically significant. Also, the results showed that though the overall level of alexithymia was higher in the female group than the male group, there was not a significant difference between the two groups.
Contrary to the findings of the present study, the study of Juha et al., where the participants’ alexithymia scores were analyzed in relation to their gender, education, marital status, and psychological disorders, reports that the level of alexithymia was significantly higher in men than in women (p<0.001), but the physical symptoms of alexithymia were more common in women than in men. Moreover, though the levels of the three subscales of EOT, DDF, and DIF were higher in men than in women, none of the differences were statistically significant (20).
Different studies report different results with regard to the prevalence of alexithymia in men and women. In their review of 32 studies, Levant et al. report that 18 studies show that, overall, men are more affected by alexithymia than women, while the other 14 studies show that there is not a significant difference between men and women in this respect(21) . The results in this review are consistent with our study. However, in our study, critical thinking was higher in men than in women. Women were also more experienced in describing and identifying feelings than were men. Women generally feel more responsible about problemswithin the family, and have more guiltyfeelings about infertility.In their respective studies, described alexithymia as a gender-dependent construct and report its prevalence to be relatively higher in men than in women (22), which was not consistent with the results of the present study, where the overall incidence of alexithymia was found to be higher in women than in men.
The results of the present study also indicate that, when the cause of infertility is unknown, the frequency level of the subscales of alexithymia is higher in both sexes. This may be because the outcome of treatment in unknown causes is not predictable.
Peterson et al. report that in cases of male infertility, there is reduction in psychological disorders in. In other studies, too, when husbands are responsible for infertility, their anxiety levels are higher than their wives’ levels(20). These results weren’t confirmed by our study.
Moreover, the results show that the frequency of alexithymia is highest in women who have been infertile for 10 to 15 years.
Our results also showed that the overall level of alexithymia in women was higher than in men. This may be because a greater responsibility of this problem falls on women, as discussed before. An increasing duration of infertility can create more concerns and reduce hope in infertility treatment.
In their study entitled “Alexithymia in Infertile Women,” Lamas et al. conclude that the disorder is more common in infertile women than in fertile women, but there is not a significant difference in the prevalence of alexithymia between women who were infertile for an unknown reason and women with tubal (organic) infertility(23). These results are not consistent with the results of the present study. But our result is is consistent with the results of many other similar studies (24, 25)
In the present study, social anxiety levels were found to be highest when the length of infertility exceeded 10–15 years. This finding is consistent with the findings of the study by Volgsten et al., which shows that longer periods of infertility correlate with a higher incidence of psychological problems in couples; especially in male infertility, men experience greater anxiety (24).
Moreover, the results of the present study show that women display the highest percentages of the subscales of social anxiety when the causes of infertility are mixed and when women themselves are responsible for infertility. This also may be related to greater concerns about the low success of treatment in dual or mixed causes of infertility.
Evidences reported that the psychological consequences of infertility can be traced back to the cause of infertility(26-28). On the other hand, the study of Ramli et al. shows that there is no difference between anxiety levels in infertile men and women based on the cause of infertility (26). As with the present study, Drosdzol & Skrzypulec study shows that infertile women demonstrate a larger number of psychological disorders than their husbands do, especially when the cause of infertility is related to the women or is unknown (27). Similarly, Ghavi etal. reported the same results(28). This confirmed our results about the high level of social phobia in mixed causes. Both men and women need and may be responsive to treatment.
Peterson et al. report that in cases of male infertility, there is reduction in psychological disorders in. In other studies, too, when husbands are responsible for infertility, their anxiety levels are higher than their wives’ levels(20). These results weren’t confirmed by our study.
In the present study, social anxiety levels were found to be highest when the length of infertility exceeded 10–15 years. This finding is consistent with the findings of the study by Volgsten et al., which shows that longer periods of infertility correlate with a higher incidence of psychological problems in couples; especially in male infertility, men experience greater anxiety (24).
Some of our research agreed with previous studies. In Iran, as in many Islamic countries, childbearing is considered a social responsibility of women, and most women are expected to give birth soon after marriage. This belief aggravates the psychological problems that infertile women can experience, thus the need for identifying and applying psychotherapy strategies, such as counseling and effective education, as part of the treatment plans for such patients.
One of the limitations of the study was the presence of the participants in infertility clinics and their worries about the processes and results of their treatment. However, the researchers tried to minimize the influences of these factors by thoroughly explaining the objectives of the study to the participants and selecting proper locations for the participants to complete the questionnaires.
Conclusion
In view of the various psychological issues that can affect infertile men and women and subsequently lead to physical, emotional, and behavioral disorders, recognizing the problems of infertility can be helpful to health policy makers in developing effective educational programs.Also So, it is necessary that the ground is paved, in addition to infertility treatment programs, to evaluate psychological disorder in infertile couples, and training, consultation and treatment programs be considered for people,so that they can enjoy a better prognosis with infertility treatments , promote mental health despite their time consumption and high costs.
Acknowledgement
The researchers’ thanks are due to all the participants and the Infertility Center of Yazd for their cooperation and support.
Conflict of interest
None
Reference
- Berek JS. Novak s Gynecology. 14th ed Philadelphia: Lippincott Williams & Wilkins 2011.
- Ramezanzadeh F, Aghssa MM, Abedinia N, Zayeri F, Khanafshar N, Jafarabadi M. Surveying of relationship between anxiety, depression and duration of infertility. . BMC Womens Health. 2004:9-16.
CrossRef - Ramazanzadeh F, Noorbala A, Abedinia N, Naghizadeh M. Emotional adjustment in infertile couples. . Iranian Journal of Reproductive Medicine 2009;7(3):97-103.
- Mosalanejad l, Khodabakshi Koolee A. Looking at infertility treatment through The Lens of the meaning of life: the effect of group logotherapy on psychological distress in infertile women. . International Journal of Fertility and Sterility
2013;6(4):224-31. - Swart M, Kortekaas R, Aleman A. Dealing with Feelings: characterizations of trait alexithymia onemotion regulation strategies and cognitiveemotional processing. . PloS One 2009;4(6):1-7.
CrossRef - Franz M, Popp K, Schafer R, Sitte W, Schneider C, Hardt J, et al. Alexithymia in the German general population. . Soc Psychiatry Psychiatr Epidemiol 2008;43:54-62.
CrossRef - Grynberg D, Luminet O, Corneille O, Grèzes J, Berthoz S. Alexithymia in the interpersonal domain: A general deficit of empathy? Personality and Individual Differences 2010;49:845-50.
CrossRef - Waller E, Scheidt CE. Somatoform disorders as disorders of affect regulation: A study comparing the TAS-20 with non-self-report measures of alexithymia. . Journal of Psychosomatic Research Journal of Psychosomatic Research 2004;57(3):239-47 •
CrossRef - Lundh LG, Johnsson A, Sundqvist K, Olsson H. Alexithymia, memory of emotion, emotional awareness, and perfectionism. . Emotion 2002;2:361-79.
CrossRef - De Berardis D, Campanella D, Gambi F. Insight and alexithymia in adult outpatients with obsessive-compulsive disorder. . European Archives of Psychiatry and Clinical Neuroscience 2005;255(5):350-8.
CrossRef - Dalrymple KL, Herbert JD. Acceptance and Commitment Therapy for Generalized social Anxiety Disorder. Behavior Modification. . Behavior Modification. 2007;31(5):543-68 .
CrossRef - Kessler R, Berglund P, Demler O, Jin R, Walters EE. Lifetime prevalence and age-of-onest distributions of DSM-IV disorders in the National Comorbidity Survey Replication. . Arch Gen Psychiatry. 2005;62(6):593-602.
CrossRef - Ellis DM, Hudson JL. The Metacognitive Model of Generalized Anxiety Disorder in Children and Adolescents. . Clin Child Fam Psychol Rev 3. 2010;13(3):151-63.
- Williams KE, Marsh WK, Rasgon NL. Mood disorders and fertility in women: a critical review of the literature and implications for future research . Hum Reprod Update 2007;13(6):607-16.
CrossRef - Guerra D, Liobra A, Veiga A, Barri P. Psychiatric morbidity in couples attending a fertility service. . Hum Reprod 1998;13:1733-6.
CrossRef - Lamas C, Chambry J, Nicolas I, Frydman R, Jeammet P, Corcos M. Alexithymia in infertile women. J of Psycho Obstet and Gyneco 2006;27(1):23-30.
CrossRef - Conrad R, Schilling G, Langenbuch M, Haidl G, Liedtke R. Alexithymia in male infertility. Human Reproduction 2001;16(3):587–92.
CrossRef - Besharat MA. Reliability and Factorial Validity of a Farsi Version of the 20-Item Toronto Alexithymia Scale with a Sample of Iranian Students 1, 2. Psychological reports. 2007;101(1):209–220.
http://dx.doi.org/10.2466/PR0.101.5.209-220 Psychological reports 2007;101(1):209-20.. http://dx.doi.org/10.2466/PR0.101.5.209-220.
CrossRef - Mohammadim MR, Ghanizadeh A, Mohammadi M, Mesgarpour B. Prevalence of social phobia and its comorbidity with psychiatric disorders in Iran. . Depression and Anxiety 2006;23(7):405 – 11 •.
CrossRef - Juha T, Juha Veijola K, Pirkko Kokkonen P, Laksy KJ, Joukamaa M. Somatization and alexithymia in young adult Finnish population. . General Hospital Psychiatry 27 (2005. 2005;27(4):244– 9.
CrossRef - Levant RF, Hall RJ, Williams CM, Nadia T, Hasan NT. Gender differences in alexithymia. . Psychology of Men & Masculinity. 2009;10(3):190-203.
CrossRef - Abedi M. Cognitive biases in interpretation in people with social phobia3. Tehran: Iran University of Medical Sciences[dissertation]. 2003.
- Lamas C, Chambry J, Nicolas I, Frydman R, Jeammet P, Corcos M. The performance of diagnostic measures of depression in alexithymic and nonalexithymic subjects. . J Psychosom Obstet Gynaecol. 2006;27(1):23-30.
- CrossRef
- Volgsten H, Svanberg AS, Ekselius L, Lundkvist O, Poromaa IS. Prevalence of psychiatric disorders in infertile women and men undergoing in vitro fertilization treatment. . Hum Reprod 2008;23:2056–63.
CrossRef - Huppelschoten AG, van Dongen AJCM, Verhaak CM, Smeenk JMJ, Kremer JAM, Nelen WLDM. Differences in quality of life and emotional status between infertile women and their partners. . Hum Rep 2013;28(8):2168–76.
CrossRef - Ramli M, Roszaman R, Rzantee Yazmie AW, Ravindran A. A preliminary study of the psychological differences in infertile couples and their relation to the coping styles. comprehensive psychiatry. 2014;55:565-9.
- Drosdzol A, Skrzypulec V. Depression and anxiety among Polish infertile couples; an evaluative prevalence study. . J Psychosom Obstet Gynaecol. 2009;30(1):11-20.
CrossRef - Ghavi F, Mosalanejad L, Golestan M, Etebariy S, Yari N. The Investigation Holistis Stress in Infertile Women and Relation to Demographic Characteristics in Women Who Referred to Yazd Infertility Center. . Biomed Pharmacol J 2015;8(2):Available from: http://biomedpharmajournal.org/?p=1885.
Accepted on: 10 November 2016








![]()
![]()
