
Assessment of Urinary Tract Calculi with 16-MDCT: The axial versus coronal plane
1Resident of Radiology, Iran University of Medical Sciences, Tehran, Iran.
2Department of Radiology, Hasheminejad Kidney Center (HKC), Iran University of Medical Sciences, Tehran, Iran.
Corresponding Author E-mail: : smb_53@yahoo.com
DOI : http://dx.doi.org/10.13005/bbra/2298
Download this article as:
![]()
The purpose of the current study was to compare the detection rate and size measurements of urinary tract calculi on coronal reformations versus the axial plane using 16-MDCT. In this cross sectional study 100 consecutive renal colic patients were evaluated using16- MDCT with collimation 1/5, axial thickness 2mm and coronal reformat thickness 2mm. Coronal and axial view randomly reported by two radiologist and then total images the other time reported by staff. 178 stones in axial and 168 stones in coronal view were detected but the mean number of detected stones in axial view was not significantly more than coronal view(p>0/05( . In two dimensional evaluation, maximum dimension of stones (kidneys and ureter totally) in coronal view was more than axial, but the difference was not significant (p>0/05). In two dimensional evaluation, maximum dimension of ureter stones the in coronal view was significantly more than axial. In 3D evaluation, stones size craniocaudaly in axial view was significantly more than coronal (0.001). The detection of stones was not improved using coronal view compared to axial view with thin thickness. Maximum size of ureter stones using coronal reformation was better estimated than axial view.Craniocaudal size of stone was overestimated in axial view than coronal probably because of partial volume effect.
KEYWORDS:Urinary Tract Stone; Axial; Coronal
Introduction
Renal colic is one of the commonest causes of people’s resorting to the emergency service department of hospitals mostly caused by urinary tract stones (1-2). Spiral CT scan without contrast is the best way to diagnose the kidney stone. Multidetector (MDCT) scanners are capable of displaying higher-resolution and quicker pictures compared to single detector helical CT and they have enhanced multiplanar reformation (MPRs). They have transformed CT from cross-sectional trans-axial technique into 3D technique (3-10). Various studies have been conducted in order to compare axial images and coronal reconstructions. For instance, some researches have been conducted using MDCT-64 indicating that the diagnostic concordance of thoracic lesions in both axial and coronal views is equal. However, other studies point to the advantage of the coronal view in evaluating the cervical lymph nodes (11-12). Mester et al (2009) studied the coronal and axial films of 80 patients suffering from renal colic and Nephrolithiasis using MDCT-64 with 0.5 mm collimation and 5 mm axial images and 3 mm coronal reconstruction. According to their research, the frequency of observing urinary tract stones in all patients in the coronal view was much more than the axial view and the radiologists was better able to estimate the size of the stones in coronal levels than axial levels. In axial levels, the size of the vertical stones was 20% underestimated (13). Another research was conducted by MemarSadeghi et al (2007) in Germany and they studied 147 patients suspicious of kidney stone complaining about flank area pain. The technique used in this research included MDCT-4 without contrast with 1 mm collimation, 3 mm axial images and 3 and 1.25 mm coronal reconstruction. According to this study, no difference was observed in the axial and coronal views in displaying the urinary tract stones in delicate reconstructions. Concerning 3 mm reconstruction, nearly 9 stones out of 264 were not detected. According to their research, the sensitivity of the coronal view in tracing the other findings categorized in the diagnosis of flank area pain is much less than the axial view (14).
Materials and Methodology
In this cross-sectional research, CT-scan studied 100 patients with kidney stone among those suspicious of or known to have kidney stone who were introduced for further examination by the urologist since early April 2012 until late February 2012.
All the scans were performed using a Multidetector device with 16 parallel detectors (made by Siemens). These were the specifications of the device: a pich of 1.2, 1.5 collimation, 2mm axial level thickness, 2mm coronal reconstructed level thickness, 150 for the milliamper tube, and a voltage of 100 kv. None of the scans were with injected or fed contrast. The information was analyzed using PACS system (efilm).
All the information within this period which belonged to those suffering from urinary tract stone was extracted. Then Block randomization method was utilized and the digital numbers belonging to each index were divided randomly in blocks of 4 into 2 groups, namely A & B in the PACS system. A indexes were read by a radiologists with board of specialties, while B indexes were read by a senior resident. Thus, the images were read by 2 radiologists who were fully unaware of the details of patients. Each radiologist took a note of the number of stones, their sites, their dimensions, and the time spent for reading each film in the following way:
Site of the stone: if the stone was in the kidney, its position would be divided into upper, middle and lower right or left calyx.If the stone was in the ureter, its location would be divided into upj, 1.3 upper, middle, lower and uvj.
Number of stones: the number of stones was described in terms of their location.
Size of the stone: the size of the stone was measured in 3 dimensions. 2 dimensions were mentioned in the cut where the highest dimensions of the stones were observed and the third dimensions was described based on the number of cuts where the stone was observable times 2 mm (thickness of cut).
Magnification factors were used for small stones in order to measure them accurately. In the next step, all the indexes were arranged and classified based on the axial and coronal indexes and read and measured by the advising professor who fulfilled the role of a reference and filled in the questionnaire. The information was fed to SPSS v.20 and analyzed using T-test, chi-square, and Pearson correlation. The value of less than 0.05 for was considered to be significant.
The total number of the stones reported by the advising professor who acted as a reference was 178 and 168 in the axial and coronal views respectively. No significant difference was observed between the view used and the diagnosis level (P > 0.05). The average size of the stone in the 2-dimensional view in coronal images was more than the axial images, but this difference was not statistically significant (P=0.06). The average maximum size of ureter stone in the 2-dimensional view in the coronal view was more than what was observed in the axial view and the difference was significant (figures 1 & 2).
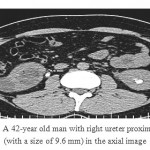 |
Figure 1: A 42-year old man with right ureter proximal stone (with a size of 9.6 mm) in the axial image.
|
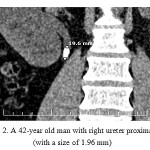 |
Figure 2: A 42-year old man with right ureter proximal stone (with a size of 1.96 mm).
|
In coronal reconstruction images, the average maximum craniocaudal length of the stone in the axial view based on the number of cuts was significantly more than the coronal view (P=0.001). No significant difference was observed in terms of observing stones under 5 mm in both views (p>0.05).
Our findings in the coronal and axial views were compared against the findings of the other radiologists in coronal and axial views. The difference in the size of the stones reported in 2D and 3D views (P>0.05) and the difference in diagnosing stones smaller than 5 mm among both groups was not significant (P=0.9).
Discussion
We utilized MDCT-16 technique here and the results were compared against one another in the axial and coronal views. The films were also masked and studied by two other radiologists. Among the 100 patients we studied, there was no significant difference in terms of detecting stone in the axial and coronal views (P=0.57). These results were in line with those of MemarSadeghi et al who showed there is no significant difference between the coronal and axial view in terms of the number of stones (14). Our results were also in line with those of Katz et al who showed that MPR and lateral view caused no significant difference in displaying the ureter stones among those patients complaining about renal colic (15). However, in the study conducted by Mester et al (2009) using axial pictures with a thickness of 5 mm and a coronal reconstruction of 3 mm, the frequency of detecting stones in coronal images was more than axial images. This may be due to using thick axial thicknesses and more delicate reconstruction resulted in the observation of more stones (13).
As the studies indicate, a coronal view results in better detection of the stones smaller than 5 mm and those stones bigger than 5 mm are observed equally in both views (3). We showed that the difference reported for the number of stones smaller than 5 mm in the axial and coronal views was not significant (P=0.3) and this is due to using delicate cuts in our study.
The average size reported by the executer of the plan and the other two radiologists in the axial and coronal views in 2D measurements of all the stones was not significant (P=0.06), although Mester et al reported that the size of vertical stones in the axial stones was measured nearly 20% less than the real size (13). This difference in conclusion can be due to the difference in the samples studied, because although this difference was not statistically significant in our study but some of the stones, especially those in the ureter, had a smaller size than the axial images. Probably, as much as our coronal images showed bigger sizes for stones, some of our axial images showed stones with bigger anteroposterior diameter and this has not made this difference significant and we need a bigger sample for better analysis. For further study, once again the difference between the biggest stone size in both views was calculated only for ureter stones and the size of the ureter stone was significantly larger in coronal images than what was observed in their axial counterparts (P=0.001). A nearly 40% underestimation was observed in the axial images.
The average maximum craniocaudal length of the stone in axial images based on counting the number of cuts exhibited a significant difference compared with the length of stone in coronal images and this difference was also observed in the measurement of the other 2 radiologists (P=0.03). The difference was nearly 4 mm. This difference may be partially caused by the Partial Volume Effect of the axial images which has probably resulted in more-than-real measurement of the stone length. Thus to measure the length, we’d better use coronal reconstruction or if we prefer using axial images, we need to subtract one cut from those cuts counted so as to reduce this difference to minimum.
There were also some limitations to our research. Firstly, there is no real standard concerning the existence or absence of the kidney stone. CT is the most sensitive method to measure stones and measuring the stones in an outside environment is not possible. The differences in the methods of research and devices with various specifications can lead to different results.
We may finally conclude, keeping in mind the importance of detecting stones even stones smaller than 5 mm which might be disposed automatically by themselves in hematuria patients, we need to use the least thickness possible while studying the urinary tract stones. If the stone was not observed in the axial view, we might attempt reconstructing it with less thickness. Further to recommending the utilization of delicate cuts, we must take into consideration the absorbed dose of the patient and its advantages and disadvantages.
To report the highest diameter of stone, especially in the case of the ureter stone, we need to use coronal reconstruction, while counting cuts is used in axial images to measure the length. At least one cut is put aside to remove the partial volume effect.
References
- Sidhu R, Bhatt S, Dogra VS. Renal Colic.UltrasoundClin 2008; 3: 159-170.
CrossRef - Bariol SV, Moussa SA, TolleyDA.Contemporary Imaging for the Managementof Urinary Stones. EAU Update Series 2005; 3: 3-9.
CrossRef - Chen MYM, Zagoria RJ. Can non contrasthelical computed tomography replaceintravenous urography for valuation ofpatients with acute urinary tract colic? JEmerg Med 1999; 17(2): 299–303.
CrossRef - Albani JM, Ciaschini MW, Streem SB, et al.The role of computerized tomographicurography in the initial evaluation ofhematuria. J Urol 2007; 177: 644-648.
CrossRef - Patel SA, Morar KN, Edwards MG. Aphysicians survey: Comparing CT versusIVP in the diagnosis of hematuria or renalcolic. J Radiol 2003; 1-5.
- Leyendecker JR, Gianin JW. Magneticresonance urography Abdom Imaging Onlinefirst: May, 2008.
- Zargar MA, Shaver B, Hadizadeh H, et al.MRU versus Pilogarghy in diagnosis ofupper urinary tract obstructions. IranianJournal of Urology 2003; 33(4): 27-33.
- Maher MM, Kalra MK, Rizzo S, et al.Multidetector CT Urography in Imaging ofthe Urinary Tract in Patients with Hematuria.Korean J Radiol 2004; 5: 1-10.
CrossRef - Van Der Molen AJ, Cowan NC, Mueller-LisseUG,Nolte-Ernsting CC, Takahashi S, Cohan RH; CTUrography Working Group of the European Societyof Urogenital Radiology (ESUR). CT urography:definition, indications and techniques—a guidelinefor clinical practice. EurRadiol 2008; 18:4–17
CrossRef - Reiser MF, Takashi M, Modic M, Bruenig R, eds.Multislice CT. Berlin, Germany: Springer-Verlag,2001
- Raff GL, Gallagher MJ, O’Neill WW, et al. Diagnostic accuracy ofnoninvasive coronary angiography using 64-slice spiral computed tomography.J Am CollCardiol. 2005;46:552-557.
CrossRef - Maintz D, Seifarth H, Raupach R, et al. 64-slice multidetectorcoronaryCT angiography: in vitro evaluation of 68 different stents. Eur Radiol. 2006;16:818-826.
CrossRef - Ur Metser1 2, Sangeet Ghai2, Yang Yi Ong2, Gina Lockwood3 and Sidney B. RadomskiAssessment of Urinary Tract Calculi With 64-MDCT: The Axial Versus Coronal Plane.American Journal of Roentgenology. 2009;192:1509-1513
CrossRef - Memarsadeghi M, Schaefer-Prokop C, Prokop M, et al. Unenhanced MDCT in patients with suspected urinary stone disease: do coronal reformations improve diagnostic performance? AJR 2007; 189:329; [web]W60–W64
- Katz DS, Venkataramanan N, Napel S, SommerFG.Can low-dose unenhanced multidetector CT beused for routine evaluation of suspected renal colic?AJR 2003; 180:313–315.
CrossRef
Accepted on: 04 September 2016








![]()
![]()
