

Manuscript accepted on : 16 June 2017
Published online on: --
Plagiarism Check: Yes
Occupational Musculoskeletal Disorders Among Taxi Industry Workers in Jeddah, Saudi Arabia
1Department of Environmental Science, Faculty of Meteorology, Environment and Arid Land Agriculture, King Abdulaziz University, P.O. Box 80208, Jeddah 21589, Saudi Arabia.
2Centre of Excellence in Environmental Studies (CEES), King Abdulaziz University, P.O. Box 80216, Jeddah 21589, Saudi Arabia.
3Vice Presidency of Projects, King Abdulaziz University, Jeddah 80216, Saudi Arabia.
Corresponding Author E-mail: mrehan@kau.edu.sa
DOI : http://dx.doi.org/10.13005/bbra/2483

ABSTRACT: Professional driving is associated with high rates of occupational musculoskeletal disorders (OMSDs). The objective of this study was to assess the prevalence of OMSDs among drivers and office workers of taxi industry in Jeddah city. A detailed custom-made questionnaire was used that included socio-demographic and occupational characteristics of subjects together with OMSDs prevalence rates. In this research, 173 subjects participated of which 70.5% were drivers and 29.5% were office workers. Standard Nordic Questionnaire (SNQ) was used to assess 1-year and 1-week prevalence rates of OMSDs in nine body regions. 1-year and 1-week reported prevalence rates of OMSDs among taxi drivers were 85.3 and 51.6%, while among office workers were 52.9 and 31.4%, respectively. The highest self-reported prevalence rates of OMSDs for taxi drivers were found for the lower back (60.7%) and lowest rates for the elbow (14.8%). Whereas, among office workers, the highest prevalence rates were found for the lower back and knee (29.4%) and lowest rates for feet/ankle (2.0%). The chi-square test found significant correlation between being immigrant (p=0.038), hours of driving per day (p=0.002), number of working days per week (p=0.000) with 1-year prevalence of OMSDs, While job experience (p=0.006), hours of driving per day (p=0.004) and break during work (p=0.029) showed significant correlation with perceived 1-week prevalence of OMSDs among taxi drivers in Jeddah.
KEYWORDS: Occupational musculoskeletal disorders; health risk assessment; taxi industry; health and safety; occupational health; ergonomics
Download this article as:| Copy the following to cite this article: Ahmad I, Balkhyour M. A, Abokhashabah T. M, Ismail I. M, Rehan M. Occupational Musculoskeletal Disorders Among Taxi Industry Workers in Jeddah, Saudi Arabia. Biosci Biotech Res Asia 2017;14(2). |
| Copy the following to cite this URL: Ahmad I, Balkhyour M. A, Abokhashabah T. M, Ismail I. M, Rehan M. Occupational Musculoskeletal Disorders Among Taxi Industry Workers in Jeddah, Saudi Arabia. Biosci Biotech Res Asia 2017;14(2). Available from: https://www.biotech-asia.org/?p=25929 |
Introduction
Work-related or occupational musculoskeletal disorders (OMSDs) include damages to neck, shoulders, elbows, wrist, back, hand and wrist bones, nerves, muscles and tendons, tendon sheaths, and synovial lubrication of tendon sheaths. OMSDs represent a collection of health problems that are more common in working class than the general population in society.1,2 OMSDs cause employee disability, workers reduced work competence and lost wages. In developing countries, OMSDs result in huge economic losses in terms of workers’ payment losses, health expenses, and efficiency losses.1,3-6 Complaints related to OMSDs are defined as pains, aches or discomfort experienced in different body regions that continued for at least 2 to 3 working days during the past week or year.1,7
Despite the well-documented facts that taxi drivers are more prone to musculoskeletal disorders (MSDs) than other professional drivers due to a lot of workload factors, their musculoskeletal health has not been studied extensively as compared to other drivers.8 They face special lifestyle challenges and distinctive professional demands, making them more vulnerable to MSDs, hypertension, diabetes and cardiovascular problems.6 Taxi drivers come across injury, violence threats and even murder.8,9 According to Hagen (2005) in Oslo, Norway taxi drivers of prominent taxi organizations encounter on average 40 incidences of serious violence each year [10]. About 400 taxi drivers are injured on the job annually, mostly through assaults.11 Taxi drivers are over 20 times more likely to be murdered on the job than other workers. The Bureau of Labor Statistics’ (BLS) USA data indicates that annual homicide rates for taxi drivers were 19 per 100,000 workers, 30 times more than the national average for all workers.12
According to National Institute of Occupational safety and Health (NIOSH), USA taxi drivers face many risk factors such as money exchange, operations of early morning and late night, lone working, personal public interaction.12 A study of USA drivers concluded assault, injury, violence, violence threats, crime and robbery as major risk factors, which may cause psychosocial and traumatic stress.8,13 Many physical factors causing MSDs among drivers have been documented like lifting,14 seating postures for long time,15 whole body vibration,16 psychosocial risks6,17 and injuries during collisions and accidents.18,19 Taxi drivers work in confined space which poses a postural strain on lumbar spines as have been proved through biomechanical studies. Some other work stressors in macro environment influencing taxi drivers are air pollutants violence and psychological strains.8,9
An epidemiological study of Chen et al. (2004) showed that prevalence of OMSDs is more among taxi drivers than other drivers.20 Whole body vibration is linked with extensive driving.13,20,21 More time behind wheels is a proved risk factor for inducing MSDs among taxi drivers evidenced by a Taiwan study.8,19 According to Institute of Occupational Safety and Health (IOSH) Taiwan survey study employing modified version of NMQ professional drivers experience prevalence of knee pain higher than the national average.6,8 Raanaas and Anderson (2008) conducted a survey of musculoskeletal complaints using Standardized Nordic Musculoskeletal Questionnaire (SNMQ)20 of Norway taxi drivers proved 1-year prevalence of knee pain was higher than that among the reference group from the local community (29% vs 25%, respectively).8 In a Nigerian study by Ojo et al. (2014), 77% of studied drivers reported MSDs including lower back pain (50.5%) as the most frequently cited body part among studied cohorts.22 Taxi drivers are subjected to lengthy periods of relative inactivity while sitting and driving together with having to do high physical work often loading, unloading, securing and tire chains installation. Furthermore, sitting for longer hours in the small space subjects drivers to full body vibration, which is undoubtedly a risk factor for musculoskeletal problems especially lower back pain problems.16,23 The vulnerability of this occupational group would be even higher in Jeddah due to harsh climatic, geographic and working conditions as well as their sociodemographic background as the majority of drivers are migrants.
There is no study published on prevalence of OMSDs in taxi industry workers in Jeddah city. The aim of this study was to assess the prevalence of OMSDs among taxi drivers and office workers in Jeddah, Kingdom of Saudi Arabia (KSA). Moreover, the risk factors to MSDs such as age, driving hours and days, sleep times, rest breaks, marital status, ethnicity, insurance facilities, and psychosocial hazards are discussed. The research outcomes are important for ergonomists, OSH practitioners, drivers, transportation unions and associations, researchers and other stakeholders. An ergonomic based intervention program can be developed on the basis of the study findings.
Materials and Methods
Instrument
Information on the prevalence and pattern of OMSDs was obtained from participants using the Standardized Nordic Questionnaire (SNQ).24 The SNQ included a drawing with nine anatomical regions clearly marked. Respondents were asked if they “ever had trouble in the past 1 year (ache, pain, or discomfort)” around five different upper quadrant body regions (neck, shoulder, elbow, wrist/hand, and upper back) and four different lower quadrant body regions (lower back, hip/thigh, knee and ankle/feet). Similarly, respondents were also asked to report the 1 week perceived trouble (ache, pain or discomfort). Furthermore, respondents who had such troubles in the past 1 year were asked if such troubles prevented them from doing their normal job, so to measure the job lost days due to perceived MSDs. Point prevalence (1 week) and period prevalence (1 year) were reported by subjects. Number of hospital/doctor visits by respondents due to MSDs were also asked to report in the custom based supplementary questionnaire.
A pre-validated standardized Nordic Musculoskeletal Questionnaire (NMQ) was used for this survey study.24 Along with custom developed demographic based supplementary questionnaire to gain the data on different influences and possible risk factors for MSDs. The survey method is a popular and common strategy in social sciences.25,26 Although assessing MSDs using NMQ is not as valid as clinical examination, but it has been used widely and its validity and reliability is acceptable and has been tested and reported in many studies.27 NMQ questionnaire has been developed by Nordic researchers for screening MSDs, as a part of ergonomic programs and for epidemiological studies of MSDs.24 Numerous studies have used a modified form of standardized NMQ28,29 and proved it to be an accepted and reliable method for assessment of MSDs.1,19,20,24,30-33 Also, a translated version of NMQ has been used in many studies and found reliable and valid.1,34,35 A pilot study was conducted to validate the process, to identify challenging elements and to review ease, clarity and questionnaire completion average time.36 The reliability of the questionnaire was checked with Corn Balch test the alpha value of trial was 0.562, which indicates that the variance of scores is reasonable.37
In our study, the custom-made questionnaire contains different socio-demographic, personal and occupational questions to screen out the effect of different factors on the OMSDs of taxi drivers and office workers. Socio-demographic data (nationality, age, educational level, working experience, marital status, resident status, insurance facilities and taxi ownership) were recorded and weight and height of participants were measured for BMI using standard methods.38 Exposure to driving was covered by the questions: working days per week and working hours per day. Smoking was not included because it is unlawful to smoke in taxi according to local regulations of KSA, so drivers don’t smoke in their taxis. Possible questions about socioeconomic status or income, an experience of violence, threatened being attacked while at work could not be included as being too sensitive and intrusive of privacy.
Study Participants
Taxi drivers and office workers (managers, clerks, helpers, mechanics, sweepers and owners) in the taxi industry having similar socio-demographic background were included in this study. The following conditions were set for participants to become study part. Only those drivers who are full-time drivers, having at least 1-year experience, aged 18 years or above, who gave informed consent, who have no history of musculoskeletal surgeries, joint replacements, musculoskeletal problems (i.e. scoliosis, kyphosis), inflammatory diseases and rheumatoid arthritis.
We employed nonexperimental, non-clinical case-control quantitative study to ascertain if there is any relationship exists between set variables and ascertain a cause and effect between these variables in relation to perceived or actual OMSDs whether work exacerbated or work related amongst taxi drivers and office workers.39 We used self-administered as well as assisted questionnaire completion method being most suitable for the descriptive method of data collection, this is confidential, accurate as well as yield greater results.36
Study Area
KSA is one the most devout and wealthiest country in the world.40 Due to economic boom and development works in previous decades, transportation sector has become a good economic sector employing around 363 thousand persons, where drivers make a substantial part.41 Jeddah, the second largest industrial and developed city of KSA, having estimated population of around 4.03 million, where expatriates are more than the local population.42 It is the administrative head quarter of Makkah Mukarramah region.43 In KSA, there are around 1,357 taxi companies, with 43,000 taxis, 33% of which are running on Jeddah roads.44 Jeddah being gate to Makkah, the holiest site in Islam is full of worshippers round the year, so taxi business is good and attracts many. Jeddah is the main gate of pilgrimage and visitors to KSA, situated at Eastern Coast of the Red Sea at Latitude 29.2º North and Longitude 39.7º East.43
Driving is a risky occupation as evidenced by stated facts. So the drivers are more prone to safety and health hazards than many other sectors in KSA and more prone than drivers in other part of the world. Most taxi drivers are Indian, Pakistani or Yemeni nationals.44 Drivers work day and night with the only purpose of earning bread and living. This makes them a one of the most vulnerable occupational groups to study. This is the first kind of its study not only in Jeddah but in KSA.
Data Collection
An introduction letter, having study details and permission for conducting the study was taken and approved by the department of Environmental Sciences, Faculty of Meteorology, Environment and arid Land Agriculture, King Abdulaziz University (KAU), Jeddah. This study was reviewed and approved by the Institutional Review Committee of Faculty of Meteorology, Environment and Arid Land Agriculture and Research Ethics Committee KAU Hospital, Jeddah KSA.
A risk assessment was made prior to study for the safety of researchers and study subjects. Each driver was individually briefed in their native language (Urdu or Arabic) regarding questions, the purpose of study and making them assured of their particulars anonymity. Almost 80% of the study subjects were native Urdu speaking from South East Asia, questionnaires were filled by participants under the supervision of leading author a native Urdu speaker. Each and every question of the questionnaire was briefed in a non-leading manner to maintain interpretation standardization. Even some additional questions were asked to subjects for making answer/response more representative. Some subjects who were graduate and knew the English language well, SNQ were self-administered to them, under the researcher supervision. Urdu version of SNQ is not available, although SNQ translated versions have been successfully used in many studies.1,34,35
Data Analysis
IBM version of SPSS Statistics 20.0 (IBM Corp., Armonk, NY, USA) was used for data analysis. Data were summarized using descriptive statistics including max, min, mean, and distribution frequency were used for summarizing data results. Chi-square test was used to study the associations between OMSDs prevalence and each of sociodemographic and occupational factors. The significance level (p-value) was set at 0.05.
Results
Response Rate, Demographics, and Personal Factors
We contacted 225 study subjects, including taxi drivers and office workers. 25 denied participation while 14 terminated study for personal reasons and 13 responses were incomplete so excluded from the study. Leaving 173 complete and evaluable questionnaires, indicating a response rate of 76.9% (Figure 1). The percentage of employee taxi drivers, owner drivers and office workers were 59.5% (103), 11% (19) and 29.5% (36) respectively. The participant’s age range was 18-30 (28.9%), 31-40 (52.0%) and above 40 (19.1%). Among the subjects, 77.3% were immigrant and 22.7 % were local residents, their education level was as primary 35.8%, secondary 54.3%, and college level 9.8%. 75.7% were married, 13.3% were unmarried and 11% were divorced/widowed. The job experience of 32.4% study subjects was between 1-10 years, 48.0% between 11-20 years and 19.7% had more than 20 years of experience, as shown in Table 1.
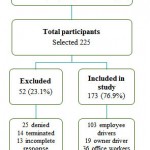 |
Figure 1: Flow chart for study subjects selection
|
Table 1: Socio demographic characteristics of Cohorts.
| Personal characteristics | N (%) | |
| Job type | Employee drivers | 103 (59.5) |
| Owner drivers | 19 (11.0) | |
| Office Worker | 51 (29.5) | |
| Age of subjects | 18-30 | 50 (28.9) |
| 31-40 | 90 (52.0) | |
| More than 40 | 33 (19.1) | |
| Residence status | Immigrant | 133 (77.3) |
| Local | 39 (22.7) | |
| Education level | Primary | 62 (35.8) |
| Secondary | 94 (54.3) | |
| College | 17 (9.8) | |
| Job experience | 1-10 | 56 (32.4) |
| 11-20 | 83 (48.0) | |
| More than 20 | 34 (19.7) | |
| Marital status | Unmarried | 23 (13.3) |
| Married | 131(75.7) | |
| Divorced | 19 (11.0) | |
| Hours of sleep per day | 5 or less than 5 | 13 (7.5) |
| 6 | 78 (45.1) | |
| 7 or more than 7 | 82 (47.4) | |
Occupational Factors
The occupational characteristics such as working days per week, working hours per day, breaks, job satisfaction and stress levels together with body weight and heights for both drivers and office workers are given in table 2. It was found that 80.3% taxi drivers work 7 days a week whereas only 7.8% office workers work for 7 days a week, while 86.3% office workers work 6 days a week. Among taxi drivers 68.0% work more than 12 hours per day while no office worker works more than 12 hours per day, 54.9% of office workers work only 8-10 hours daily. Job satisfaction level was higher (74.5%) amongst office workers than taxi drivers (47.5%). Similarly, the work stress levels were higher in taxi driver than office workers, 35.3% reporting having stress often and 50.9% sometimes, compared with 21.6% and 45.1%, respectively. The average weight and height of drivers and office workers were 91.1 and 85.3 kg, 170.9 and 171.6 cm, while average BMI for both groups were 26.74 and 24.88 respectively. A brief breakdown of the study cohorts’ responses is given in table 2.
Table 2: Occupational characteristics results of cohorts.
| Occupational characteristics | Drivers | Office workers | |
| N (%) | N (%) | ||
| Work days per week | 5 | 4 (3.3) | 3 (5.9) |
| 6 | 20 (16.4) | 44 (86.3) | |
| 7 | 98 (80.3) | 4 (7.8) | |
| Work hours per day | 8-10 | 10 (8.2) | 28 (54.9) |
| 10-12 | 29 (23.8) | 23 (45.1) | |
| More than 12 | 83 (68.0) | 0 (0.0) | |
| Job satisfaction | No | 64 (52.5) | 13 (25.5) |
| Yes | 58 (47.5) | 38 (74.5) | |
| Work stress | Often | 43 (35.3) | 11 (21.6) |
| Sometimes | 62 (50.9) | 23 (45.1) | |
| No | 17 (14.0) | 17 (33.3) | |
| Break during Job | 82 (67.2) | 43 (84.3) | |
| Weight kg (mean) | 91.05 | 85.25 | |
| Height cm (mean) | 170.9 | 171.6 | |
| BMI kg/m2 (mean) | 26.74 | 24.88 | |
Prevalence Rate of Occupational Musculoskeletal Disorders (OMSDs)
Among taxi drivers, the estimated 1-year prevalence of MSDs was 85.3% (i.e., 104 out of 122) while 1-week prevalence was 51.6%. Also the prevalence of the different MSD domains were lower back pain (60.7%), neck (52.5%), knee (46.7%), upper back (38.5%), shoulder (37.7%), thigh (36.9%), feet/ankle (18.9%), hand/wrist (18.0%) and elbow (14.8%) pains as shown in Figure 2. Among office workers, the estimated 1-year prevalence of MSDs was 52.9% while 1-week prevalence was 31.4%. Also the prevalence of the different MSD domains were lower back pain (29.4%), Knee (29.4%), Neck (27.6%), upper back (23.5%), shoulder (20.0%), thigh (11.8%), Hand/wrist (3.9%), elbow (3.9%) and feet/ankle (2.0%) (Table 3).
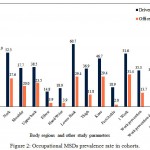 |
Figure 2: Occupational MSDs prevalence rate in cohorts.
|
Table 3: Occupational MSDs prevalence rate in cohorts.
| Prevalence rate | Drivers
N (%) |
Office workers
N (%) |
| 1 Year | 104 (85.3) | 27 (52.9) |
| Neck | 64 (52.5) | 14 (27.6) |
| Shoulder | 46 (37.7) | 10 (20.0) |
| Upper back | 47 (38.5) | 12 (23.5) |
| Elbow | 18 (14.8) | 2 (3.9) |
| Hand/Wrist | 22 (18.0) | 2 (3.9) |
| Lower back | 74 (60.7) | 15 (29.4) |
| Thigh | 45 (36.9) | 6 (11.8) |
| Knee | 57 (46.7) | 15 (29.4) |
| Feet/Ankle | 23 (18.9) | 1 (2.0) |
| 1 Week | 63 (51.6) | 16 (31.4) |
| Work prevention | 43 (35.3) | 7 (13.7) |
| Work prevention days | 42 (34.4) | 5 (9.8) |
| Hospital visits | 44 (36.1) | 6 (11.7) |
The 1-year (period prevalence) data indicates that in the lower quadrant of body lower back disorders (60.7%) were the most common reported MSD among taxi drivers. Further in the lower quadrant knee (46.7%), thigh (36.9%) and feet/ankle (18.9%) were commonly affected as reported by drivers. The period prevalence rate of lower back disorders was significantly associated with drivers work stress (p=0.018) only, the drivers with more work stress affected more and vice versa other socio-demographic and professional parameters were not significantly associated with lower back disorders. Also the period prevalence of OMSDs in the thigh was significantly associated (p=0.028) with age of drivers. Likewise, period prevalence of OMSDs in knee was significantly associated (p=0.042, 0.001, 0.009) with resident status, work hours and work stress respectively as shown in table 4.
Table 4: Prevalence of lower quadrant OMSDs among drivers and their association with personal and occupational factors.
| Factors | Lower back | Hip/thigh | Knee | Ankle/feet | ||||||||
| N | % | p | N | % | p | N | % | p | N | % | P | |
| Job type
Employee driver Owner driver |
65 9 |
63.1 47.4 |
0.197 |
38 7 |
36.9 36.8 |
0.997 |
50 7 |
48.5 36.8 |
0.384 |
20 3 |
19.4 15.8 |
0.710 |
| Ag(y)
18-30 31-40 Above 40 |
24 35 15 |
57.1 61.4 65.2 |
0.806 |
14 17 14 |
33.3 29.8 60.9 |
0.028 |
21 25 11 |
50.0 43.9 47.8 |
0.827 |
8 9 6 |
19 15.8 26.1 |
0.566 |
| Residence
immigrant Local |
60 13 |
62.5 52.0 |
0.339 |
35 9 |
36.5 36.0 |
0.966 |
47 10 |
49.0 40.0 |
0.042 |
19 4 |
19.8 16.0 |
0.667 |
| Experience
1-10 11-20 Above 20 |
22 35 17 |
47.8 70.0 65.4 |
0.073 |
13 20 12 |
28.3 40.0 46.2 |
0.267 |
16 28 13 |
34.8 56.0 50.0 |
0.107 |
7 10 6 |
15.2 20.0 23.1 |
0.689 |
| Work Break
Yes No |
50 24 |
61.0 60 |
0.918 |
12 13 |
30 40.2 |
0.271 |
40 17 |
48.8 42.5 |
0.514 |
17 6 |
20 15 |
0.447 |
| Work days
5 6 7 |
1
9 64 |
25.0
45.0 65.3 |
0.079 | 0
8 37 |
0
40 37.8 |
0.293 | 1
7 49 |
25
35 50 |
0.319 | 1
3 19 |
25.0
15.0 19.4 |
0.856 |
| Work / day
8-10h 11-12h Above 12h |
4 13 57 |
40.0 44.8 68.7 |
0.29 |
5 7 33 |
50 24.1 39.8 |
0.217 |
5 5 47 |
50.0 17.2 56.6 |
0.001 |
3 4 16 |
30.0 13.8 19.3 |
0.520 |
| Work stress
Often Sometimes |
28 41 |
65.1 66.1 |
0.018 |
14 27 |
32.6 43.5 |
0.243 |
18 36 |
41.9 58.1 |
0.009 |
8 13 |
18.6 21.0 |
0.690 |
Interestingly job type (employee drivers, owner drivers), working experience, work break observed and working days per week were not associated significantly with lower quadrant OMSDs.
The period prevalence results showed that in the upper quadrant of neck disorders (52.5%) were the most common reported MSD among taxi drivers. The other effected body regions in the upper quadrant are upper back (38.5%), shoulder (37.7%), hand/wrist (18.0%) and elbow (14.8%). As shown in table 5. The period prevalence rates in the most commonly reported upper body quadrant of neck were not significantly associated with any socio-demographic and occupational characteristics. The prevalence rate in upper back was significantly associated with work experience (p=0.003) and rest breaks (p=0.011) observed by drivers. Also, period prevalence of OMSDs in wrist/hand was nearly significant (p=0.057) with rest breaks. The drivers who observe rest breaks are less likely to have OMSDs than the drivers who don’t rest while at the job.#
Table 5: Prevalence of upper quadrant OMSDs among drivers and their association with personal and occupational factors.
| Factors | Neck | Shoulder | Upper Back | Elbow | Wrist/Hand | ||||||||||
| N | % | p | N | % | p | N | % | p | N | % | p | N | % | p | |
| Job type
Employee driver Owner driver |
54 10 |
52.4 52.6 |
0.987 |
39 7 |
36.9 37.8 |
0.933 |
39 8 |
37.9 42.1 |
0.727 |
15 3 |
14.6 15.8 |
0.890 |
19 3 |
18.4 15.8 |
0.782 |
| Age (y)
18-30 31-40 Above 40 |
24 24 16 |
57.1 42.1 69.6 |
0.063 |
13 23 10 |
31.3 40.4 43.5 |
0.519 |
14 21 12 |
33.0 36.9 52.8 |
0.308 |
8 6 4 |
19.0 10.5 17.4 |
0.460 |
8 9 5 |
19.0 15.8 21.7 |
0.804 |
| Residence
Immigrant Local |
51 13 |
53.5 52.0 |
0.920 |
38 7 |
39.6 28.0 |
0.286 |
37 10 |
38.5 40.0 |
0.894 |
14 3 |
14.6 12.0 |
0.741 |
17 4 |
17.7 16.0 |
0.841 |
| Experience
1-10 11-20 Above 20 |
19 27 18 |
41.1 44.0 69.2 |
0.072 |
15 22 9 |
32.6 44.0 34.6 |
0.482 |
10 21 16 |
21.7 42.0 61.5 |
0.003 |
8 5 5 |
17.4 10.0 19.2 |
0.457 |
7 11 4 |
15.2 22.0 15.4 |
0.637 |
| Work Break
Yes No |
19 45 |
47.5 54.9 |
0.444 |
32 14 |
39.0 35.2 |
0.667 |
38 9 |
46.3 22.5 |
0.011 |
13 5 |
15.9 12.5 |
0.624 |
11 11 |
13.4 27.5 |
0.057 |
| Work days
5 6 7 |
2 9 53 |
50.0 45.0 54.1 |
0.756 |
1 6 39 |
25 30 39.8 |
0.618 |
1 7 39 |
25.0 35.0 39.8 |
0.786 |
1 2 15 |
25.0 10.0 15.3 |
0.699 |
0 4 18 |
0.0 20.0 18.4 |
0.625 |
| Work hours/ day
8-10 11-12 Above 12 |
6 13 45 |
60.0 44.8 54.2 |
0.604 |
2 10 34 |
20 34.1 41.8 |
0.399 |
4 9 34 |
40.0 31.0 41.0 |
0.636 |
2 4 12 |
20.0 13.8 14.5 |
0.884 |
1 5 11 |
10.0 17.2 19.3 |
0.765 |
| Work stress
Often Sometimes |
21 37 |
48.8 59.7 |
0.171 |
15 25 |
34.6 40.5 |
0.832 |
17 26 |
39.5 41.9 |
0.380 |
6 10 |
14.0 16.1 |
0.889 |
8 12 |
18.6 19.4 |
0.765 |
Activity Limitation and Hospital Visits
Work prevention and activity limitation due to OMSD was 35.3% and 13.7% among drivers and office workers respectively. Also, 34.4% drivers and 9.8% office workers reported work prevention days in 1-year due to OMSDs. Hospital or doctor visits for redressal of OMSDs were 36.1% and 11.7% among drivers and office workers respectively.
Determinants of MSDs
In Pearson chi-square test being immigrant (p= 0.038), hours of driving per day (p=0.002), number of working days per week (p=0.000) were found to be significantly associated with 1-year prevalence of MSDs among taxi drivers while job experience (p=0.006), hours of driving per day (p=0.004) and break during work (p=0.029) were the significant variables which shows significant association with perceived 1 week MSDs prevalence among taxi drivers in Jeddah.
Discussion
Current research objective was to determine the frequency of OMSDs in taxi drivers and office workers and further to investigate the association of some risk factors with MSDs in taxi drivers. Study results revealed that prevalence of MSDs in cohorts are very high and more than half of cohorts experienced MSDs in the last 1 year. In this study, taxi drivers were more likely to develop MSDs as compared to office workers in taxi industry. The 1-year prevalence rate for drivers was 85.3%, while it was 52.9% for office workers. Similarly 1 week (point) prevalence rates for drivers and office workers were 51.6% and 31.4% respectively.
The highest pain reported body region was lower back (60.7%), while the lowest reported region was elbow (14.8%) among drivers in last 1 year. Whereas, the maximum and minimum pain reported regions for office workers were lower back (29.4%) and ankle/feet (2.0%) respectively. The findings from our study are in agreement with various other studies.1,32,45 Our study findings indicates that drivers experience more MSDs than office workers in the last one year as well as last one week. It can be explained that more disorders in drivers may be due to physical work load i.e. handling of luggage etc. prolonged driving duration, repetitive movements, forceful exertions, prolonged sitting in a micro taxi environment, whole-body vibration, and psychological occupational stressors. Furthermore, upper extremity disorders may be the result of the arms and neck posture, repetitive upper-limb activity and hand–arm vibration.1,17,45
MSDs are exceedingly prevailing among drivers, varying between 53% and 91% in different parts of the world.8,32,46,47 However, no study has been done on this occupation in KSA. Besides the fact that this is a highly vulnerable occupational group due to many reasons like being immigrant, they work as self-employed, they work 7 days a week, most of them work more than 12 hours, and they work round the year in an air conditioned taxi as the average temperature didn’t fall below 30°C round the year. Some other challenges related to this occupation in KSA are heavy traffic and high accidents rates as reported by Mansuri (2015).48 According to study road traffic accidents accounts for 19 deaths daily, and 4 injuries every hour.48,49 Road traffic fatalities are more than Australia, UK and USA48 which claim 4.7% mortalities of all mortalities. The country ranks high in the accident to death ratio in high-income countries and is considered to be the one of the main cause of death for 16-30-year-old males.50,51 All these facts make driving a risky occupation which can cause psychosocial hazards and risks for drivers.
In this study, disorders in lower back pain were the highest reported prevalent symptom, occurring in 60.7% of the taxi drivers in Jeddah. This prevalence rate is higher than the prevalence rates (45.8–59%) reported among Caucasians8,19,21,52 and among African where the prevalence rates were found to be between 30.7-34.3%.53,54 Increased probability of developing MSDs with increased driving duration in hours per day, as well as working days per week, were observed among the participants in this study was significantly associated with increased risk of MSDs. The drivers in Jeddah reported that they work for longer durations (80.3% work 7 days a week, 68.0% work daily more than 12 hours) while sitting in fixed position in a relatively confined uncomfortable place and vibrating taxi environment. Moreover driving seat offers little room for flexing and movement of the limbs, causing postural strain on the musculoskeletal system. This can be uncomfortable and stressing and thus aggravating susceptibility to MSDs. Many researches on occupational driver’s proved the association between MSDs and long hours and duration of driving. For example, a Taiwan study of Taipei taxi drivers reported that driving more than 10 hours per day is significantly associated with risk of knee disorders in drivers.20 The increased prevalence of low back pain risks among taxi drivers due to longer hours have been reported by many studies like driving daily continuously more than 4 hours,19 driving weekly more than 71 hours8 and driving more than 20 hours per week55 was associated with high prevalence of low back disorders. Among drivers, the employee drivers were more likely to develop MSDs than owner drivers probably because they have less control over their working hours as reported by Abledu et al. (2014) in Ghana.54
In our study, the correlation between driving experience, work breaks during driving and OMSDs was found to be significant among taxi drivers, which is in agreement with previous reported studies.8,19 Moreover, it has been proved that psychosocial factors like work stress, job dissatisfaction etc. have important role in causing MSDs among taxi drivers.19,20 In our study, self-perceived job stress was found to have highly significant correlation with MSDs i.e. lower back disorders (p=0.018) and knee disorders (0.009) in the chi-square test, which is also in agreement with study conducted by Abledu et al. (2014).54 Taxi drivers may perceive stress while on road due to dangerous driving activities like speeding, sudden stops and speaking on the phone while driving by other vehicle drivers on road etc.44
Generally, taxi companies in Jeddah charge the drivers around SR150 ($40) per day on average as their share for providing the car and other facilities. However, various drivers reported that they are not able to submit such amounts sometime, consequently build the stress of being fired. The drivers also reported that sometimes they have to pay for the damages in case of accident or traffic violations from their own pocket, which cause extra stress especially amongst immigrant drivers. Furthermore, other challenges other psychosocial factors such as being immigrant, job stress and home sickness may aggravate the prevalence of OMSDs in Jeddah taxi drivers. Contrary to reports in literature the BMI Index and weight were not significantly associated with OMSDs as having been cited in the cross-sectional and cohort studies.56,57 This may be attributed to sampling, methodological and population differences.
Limitations
The current study depends on subjective reporting for estimating the prevalence of MSDs which can possibly be biased in some cases. Furthermore, objective information regarding nature of perceived MSDs, like reported MSDs sidedness, the clinical significance of the association between MSDs and driving hours, was unavailable. Future studies should cover these limitations, particularly investigation of MSD in relation to early osteoarthritis and subsequent disability among occupational drivers. The methodology can be further enhanced considering other related studies.58-61 As the study was conducted in the winter season, due to harsh climatic and hot weather conditions in summer the perceived MSDs symptoms might vary among study subjects. Shortcomings of the employed cross-sectional design can be another limitation. Even though we did employ a widely accepted and reliable NMQ, it lacks comprehensive items for assessment of MSDs severity. Also being questionnaire-based survey; it might reflect attitude and perception of participants for reporting musculoskeletal symptoms. Thus, the perceived prevalence of OMSDs among study subjects in other regions might be different having diverse attitudes and perception even though exposed to a similar level of hazards and risks.
Recommendations
In order to protect driver’s health, they need to be educated regarding ergonomics, risks of continuous driving for long hours and not having regular breaks, the motivation for physical exercise, maintaining BMI and adaptation of healthy living styles. For drivers, interventional plans should be advocated which help in preventing or decreasing OMSDs, these may include, education, awareness, good sleep, use of ergonomically designed seat cushions, regular medical checkups and early detection and management of OMSDs. At the national level, identifying and assigning work-related diseases costs could outcome in substantial savings for the National Health System. This even can offer an incentive for the prevention of such preventable reasons of diseases and hence contribute to the sustainability of social systems. Randomized clinical trials on the effects of personal and professional factors on OMSDs are required.
Conclusion
The estimated 1-year prevalence rates of MSDs were found to be 85.3% among taxi drivers, while 1-week prevalence was 51.6%. Also the prevalence of the different MSD domains were lower back pain (60.7%), neck (52.5%), knee (46.7%), upper back (38.5%), shoulder (37.7%), thigh (36.9%), hand/wrist (18.0%), feet/ankle (18.8%) and elbow (14.7%). Among office workers, the estimated 1-year prevalence rates of MSDs was 52.9% while 1-week prevalence was 31.7%. Also the prevalence of the different MSD domains were lower back pain (29.4%), knee (29.4%), neck (27.4%), upper back (23.5%), shoulder (20.0%), thigh (11.8%), hand/wrist (4.0%), elbow (3.9%) and feet/ankle (2.0%). Work prevention and activity limitation due to OMSD was 35.2 and 13.7% among drivers and office workers respectively. The study found high levels of MSDs among taxi drivers in Jeddah, associated with age, long working hours, residence status, more working days, longer work experience, perceived job stress and breaks during the job. These findings call for preventive strategies and safety guidelines in order to reduce the incidence of MSDs in urban taxi drivers in Jeddah. This cross-sectional study provides the baseline for elaborative studies in the future. Occupational safety and health management intervention should be carried out to avoid adverse health effects among study subjects.
Acknowledgments
This article was funded by the Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah. The authors therefore acknowledge with thanks DSR for technical and financial support. We are thankful to all taxi industry managers, drivers, and office workers for their cooperation, time and thoughtful comments.
References
- Mozafari A.,Vahedian M.,Mohebi S.,Najafi M. Work-related musculoskeletal disorders in truck drivers and official workers. Acta Med. Iranica. 2015;53:432-438.
- Saldaña N. Active Surveillance of Work-Related Musculoskeletal Disorders. In Occupational Ergonomics: Theory and Applications, Second Edition, CRC Press: 2012;555-568.
- Arndt V., Rothenbacher D.,Daniel U.,Zschenderlein B.,Schuberth S.,Brenner H. Construction work and risk of occupational disability: a ten year follow up of 14 474 male workers. Occup. Environ. Med. 2005;62:559-566.
CrossRef - Meerding W. J.,IJzelenberg W.,Koopmanschap M., Severens J. L.,Burdorf A. Health problems lead to considerable productivity loss at work among workers with high physical load jobs. J. Clin. Epidemiol. 2005;58:517-523.
CrossRef - Apostolopoulos Y.,Sönmez S.,Shattell M. M.,Belzer M.,Guo H. R.,Chang Y. C.,Yeh W. Y., Chen C. W.,Guo Y. L. Worksite-induced morbidities among truck drivers in the United States. AAOHN J. 2010;58:285-296. Prevalence of musculoskeletal disorder among workers in Taiwan: a nationwide study. J. Occup. Health. 2004;46:26-36.
CrossRef - Aghilinejad M.,Choobineh A.,Sadeghi Z.,Nouri M. Prevalence of musculoskeletal disorders among Iranian steel workers. Iran Red Crescent Med. J. 2012;14:198-203.
- Raanaas R. K.,Anderson D. A questionnaire survey of Norwegian taxi drivers’ musculoskeletal health, and work-related risk factors. Int. J. Ind. Ergon. 2008;38:280-290.
CrossRef - Barish R. C. Legislation and regulations addressing workplace violence in the United States and British Columbia. Am. J. Prev. Med. 2001;20:149-154.
CrossRef - Hagen T. Improved Safety in Public Transport. A Guide with Examples of Programmes of Action. 2005.
- Work Safe Victoria, A Health and Safety Solution. https://www.worksafe.vic.gov.au /data/assets/pdf_file/0014/14027/hss_taxi_driver_web.pdf (accessed on 20 January 2017).
- National Institute for Occupational Safety and Health (NIOSH). A recent increase in homicides, taxi drivers, Anchorage, Alaska. https://www.cdc.gov/niosh/nioshtic-2/20033914.html (accessed on 20 January 2017).
- Krause N., Ragland D. R.,Greiner B. A.,Fisher J. M.,Holman B. L.,Selvin S. Physical workload and ergonomic factors associated with prevalence of back and neck pain in urban transit operators. Spine. 1997;22:2117-2126.
CrossRef - Massaccesi M.,Pagnotta A.,Soccetti A.,Masali M.,Masiero C.,Greco F. Investigation of work-related disorders in truck drivers using RULA method. Appl. Ergon. 2003;34:303-307.
CrossRef - Sadeghi N.,Habibi E.,Sajjadi S. The relationships between musculoskeletal disorders and anthropometric indices in public vehicle drivers. Int. j. collab.res. internal med. public health. 2012;4:1173-84.
- Hoozemans M. J.,VAN DERBEEK A. J.,Fringsdresen M. H.,Van Dijk F. J.,Van Der Woude L. H. Pushing and pulling in relation to musculoskeletal disorders: a review of risk factors. Ergon. 1998;41:757-781.
CrossRef - Bovenzi M., Zadini A. Self-reported low back symptoms in urban bus drivers exposed to whole-body vibration. Spine 1992;17:1048-1059.
CrossRef - Hoy J.,Mubarak N.,Nelson S.,De Landas M. S.,Magnusson M.,Okunribido O.,Pope M. Whole body vibration and posture as risk factors for low back pain among forklift truck drivers. J. Sound Vib. 2005;284:933-946.
CrossRef - Chen J. C.,Chang W. R.,Chang W.,Christiani D. Occupational factors associated with low back pain in urban taxi drivers. Occ. Med. 2005;55:535-540.
CrossRef - Chen J. C.,Dennerlein J. T.,Shih T. S.,Chen C. J.,Cheng Y.,Chang W. P.,Ryan L. M.,Christiani D. C. Knee pain and driving duration: a secondary analysis of the Taxi Drivers’ Health Study. Am. J. Public Health. 2004;94:575-581.
CrossRef - Funakoshi M.,Taoda K.,Tsujimura H.,Nishiyama K. Measurement of whole-body vibration in taxi drivers. J. Occup. Health. 2004;46:119-124.
CrossRef - Ojoawo A. O.,Onaade O.,Adedoyin R.,Okonji A. Assessment of Work Related Musculoskeletal Pain among Professional Drivers in the Service of a Tertiary Institution. Am. J. Health Res. 2014;2:56-60.
CrossRef - Macfarlane G. J.,Thomas E.,Papageorgiou A. C.,Croft P. R.,Jayson M. I.,Silman A. J. Employment and physical work activities as predictors of future low back pain. Spine. 1997;22:1143-1149.
CrossRef - Kuorinka I.,Jonsson B.,Kilbom A., Vinterberg H.,Biering-Sørensen F.,Andersson G., Jørgensen K. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987;18:233-237.
CrossRef - Mark S.,Philip L.,Adrian T. Research methods for business students. Harlow: Prentice Hall. 2009.
- Sultan N. The review of prevalence of percieved work-related musculoskeletal disorders (WRMSD), namely lower back pain (LBP) amongst hackney carriage taxi drivers in birmingham, UK.
- Descatha A.,Roquelaure Y.,Chastang J. F.,Evanoff B.,Melchior M.,Mariot C.,Ha C.,Imbernon E.,Goldberg M., Leclerc A. Validity of Nordic-style questionnaires in the surveillance of upper-limb work-related musculoskeletal disorders. Scand. J. Work Environ. Health. 2007;33:58.
CrossRef - Mehrdad R.,Dennerlein J. T.,Haghighat M.,Aminian O. Association between psychosocial factors and musculoskeletal symptoms among Iranian nurses. Am. J. Ind. Med. 2010;53:1032-1039.
CrossRef - Nordin N. A. M.,Leonard J. H.,Thye N. C. Work-related injuries among physiotherapists in public hospitals a Southeast Asian picture. Clinics. 2011;66:373-378.
- Hayes M.,Cockrell D.,Smith D. A systematic review of musculoskeletal disorders among dental professionals. Int. J. Dent. Hyg. 2009;7:159-165.
CrossRef - Bergqvist U.,Wolgast E.,Nilsson B.,Voss M. The influence of VDT work on musculoskeletal disorders. Ergon. 1995;38:754-762.
CrossRef - Mansfield N.,Marshall J. Symptoms of musculoskeletal disorders in stage rally drivers and co-drivers. Br. J. Sports Med. 2001;35:314-320.
CrossRef - Hagen K. B.,Magnus P.,Vetlesen K. Neck shoulder and low-back disorders in the forestry industry: relationship to work tasks and perceived psychosocial job stress. Ergon. 1998;41:1510-1518.
CrossRef - Choobineh A.,Lahmi M.,Shahnavaz H.,Jazani R. K.,Hosseini M. Musculoskeletal symptoms as related to ergonomic factors in Iranian hand-woven carpet industry and general guidelines for workstation design. Int. J. Occup. Saf. Ergon. 2004;10:157-168.
CrossRef - Choobineh A.,Movahed M.,Tabatabaie S. H.,Kumashiro M. Perceived demands and musculoskeletal disorders in operating room nurses of Shiraz city hospitals. Ind. health 2010;48:74-84.
CrossRef - Cargan L. Doing social research. Rowman & Littlefield Publishers. 2007.
- Rocha L. P.,Cezar-Vaz M. R.,Almeida M. C. V. d.,Bonow C. A.,Silva M. S. d.,Costa V. Z. d. Use of personal protective equipment by gas stations workers: a nursing contribution. Texto & Contexto-Enfermagem. 2014;23:193-202.
CrossRef - Willett W. C.,Dietz W. H.,Colditz G. A. Guidelines for healthy weight. N. Engl. J. Med. 1999;341:427-434.
CrossRef - Burns N.,Grove S. K. The practice of nursing research. Conduct, critique & utilization. 1993;4.
- Ahmad I.,Rehan M.,Balkhyour M.,Abbas M.,Basahi J.,Almeelbi T.,Ismail I. M. Review of Environmental Pollution and Health Risks at Motor Vehicle Repair Workshops Challenges and Perspectives for Saudi Arabia. Int. J. Agric. Environ. Res. 2016;2:1-23.
- General Authority for Statistics. Available online: http://www.stats.gov.sa/en/node/ (accessed on 20 January 2017).
- Saudi Gazette http://saudigazette.com.sa/saudi-arabia/jeddah-jubail-expats-saudis/ (accessed on 26 March 2017).
- Jeddah Economic Gateway, Jeddah guide facts and figures. Jeddah Chamber of Commerce and Industry. Available online: http://www.jeg.org.sa/data/modules/contents/uploads/ infopdf/1090.pdf/ (accessed on 20 January 2017).
- Arab News. Available online: http://www.arabnews.com/news/534626 Taxi drivers find it difficult to make ends meet. (accessed on 20 January 2017).
- Andersen J.,Kaergaard A.,Mikkelsen S.,Jensen U., Frost P.,Bonde J.,Fallentin N.,Thomsen J. Risk factors in the onset of neck/shoulder pain in a prospective study of workers in industrial and service companies. Occup. Environ. Med. 2003;60:649-654.
CrossRef - Robb M. J.,Mansfield N. J. Self-reported musculoskeletal problems amongst professional truck drivers. Ergon. 2007;50:814-827.
- Akinpelu A.,Oyewole O.,Odole A.,Olukoya R. Prevalence of musculoskeletal pain and health seeking behaviour among occupational drivers in Ibadan, Nigeria. Afr. J. Biomed. Res. 2011;14:89-94.
- Mansuri F. A.,Al-Zalabani A. H., Zalat M. M.,Qabshawi R. I. Road safety and road traffic accidents in Saudi Arabia. A systematic review of existing evidence. Saudi. Med. J. 2015;36:418-424.
CrossRef - Al Turki Y. A. How can Saudi Arabia use the Decade of Action for Road Safety to catalyse road traffic injury prevention policy and interventions? Int. J. Inj. Contr. Saf. Promot. 2014;21:397-402.
CrossRef - Violence W. H. O.,Prevention I.,Organization W. H., Global status report on road safety 2013: supporting a decade of action. World Health Organization: Available online. 2013. http://www.who.int/violence_injury_prevention/road_safety_status/2013/en/ (accessed on 20 March 2017).
- Organization W. H., Global status report on road safety: time for action. Geneva: World Health Organization. 2009. Available online: http://www.who.int/violence_injury_ prevention/road_safety_status/ 2009/en/ (accessed on 20 March 2017).
- Miyamoto M.,Konno S., Gembun Y.,Xinyu L.,Minami K.,Hiromoto I. Epidemiological study of low back pain and occupational risk factors among taxi drivers. Ind. Health. 2008;46:112-117.
CrossRef - Samuel O. A.,Babajide L. E. The prevalence of work related musculoskeletal disorder among occupational taxicabs drivers in Nigeria. Int. J. Res. Rev. App Sci. 2012;11.
- Abledu J.,Offei E.,Abledu G. Occupational and personal determinants of musculoskeletal disorders among urban taxi drivers in Ghana. Sch Res. Not. 2014;2014.
- Porter J. M.,Gyi D. E. The prevalence of musculoskeletal troubles among car drivers. Occup. Med. 2002;52:4-12.
CrossRef - da Costa B. R.,Vieira E. R. Risk factors for work‐related musculoskeletal disorders: a systematic review of recent longitudinal studies. Am. J. Ind. Med. 2010;53:285-323.
- Nilsen T. I. L.,Holtermann A.,Mork, P. J. Physical Exercise, Body Mass Index, and Risk of Chronic Pain in the Low Back and Neck/Shoulders: Longitudinal Data From the Nord-Trøndelag Health Study. Am. J. Epidemiol. 2011;174: 267-273.
CrossRef - Aalizadeh A., Daneshi A., Shirkhani., et al. The effect of Short-term Plyometric Training Program on Sprint, Strength, Power and Agility Performance in non-athletic men. Biosci. Biotechnol. Res. Asia 2015;12(2):1389-1395.
CrossRef - Koshkaki R. R., Poorgholami F., Jahromi M. K., Koshkaki A. R. A Study of the Status of Environmental Health at the Junior High-schools. Biosci. Biotechnol. Res. Asia 2016;13(4):2307-2311.
CrossRef - Koshkaki A. R., Pishgar Z., Jahromi M. K., Ramezanli S. A Study of the Awareness of the Nursing Students with the Ethical Codes of Clinical Care at Jahrom University of Medical Sciences. Biosci. Biotechnol. Res. Asia. 2016;13(4):2125-2129.
CrossRef - Maher H. S., Babaeer A. L., Awfi M. S. H. Prevalence Study of Hepatitis A Virus (HAV) on Jeddah Population. Biosci. Biotechnol. Res. Asia. 2011;8(2):585-590.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.



