
Osteo-Nevus of Nanta (Osseous Metaplasia in an Intradermal Melanocytic Nevus): Case Report of an Uncommon Phenomenon
Download this article as:
![]()
Many interesting histopathological changes may be seen in association with nevi, such as amyloid, nodular myxoid changes, folliculitis, granular cell changes and ossification. We report unusual case of osseous metaplasia within an intradermal melanocytic nevus, osteo-nevus of Nanta. Oral and Maxillofacial pathologist should be aware of this rare entity as they might receive skin biopsy from facial and perioral regions. The possible pathogenesis hypotheses have been discussed briefly.
KEYWORDS:Osteo-Nevus of Nanta; Osseous Metaplasia; Intradermal Melanocytic Nevus
Introduction
Bone formation in the skin has traditionally been classified into two types; a primary form in which there is absence of a pre-existing lesion and a secondary form where ossification develops in association with inflammatory, traumatic, and neoplastic lesions.1 The secondary ossification has been reported in pilomatricoma, basal cell carcinoma, and acne vulgaris. 2 3 Ossification in association with melanocytic nevi (osteo-nevus of Nanta) is uncommon phenomena and mostly in lesions from the face. 2 4 We report a case of osteo-nevus of Nanta and discuss its pathogenesis and significance.
Case Report
A 40 year old Saudi female presented to Oral Medicine Clinic in Al Yammamh Hospital, Riyadh with an enlarging mole on the right side of the face. The biopsy tissue received at histopathololgy laboratory, College of Dentistry, King Saud University, consisted of an ellipse of skin (2.4X 1.5X 0.7 cm) with a dark grayish center. Microscopic examination revealed a benign intradermal melanocytic proliferation exhibiting normal maturation pattern (Figure1). There was focal folliculitis and stromal chronic inflammation. Dysplastic or malignant changes was not evident. Deep within the dermis and beneath the nevus cells, rings of lamellar bone were present (Figure2). There is prominent osteoblastic rimming with a thin layer of osteoid at the outer shell of the rings, with focal osteoclastic activity. (Figure3) A diagnosis of osseous metaplasia in an intradermal melanocytic nevus (osteo-nevus of Nanta) was made.
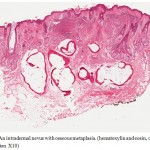 |
Figure 1: An intradermal nevus with osseous metaplasia. (hematoxylin and eosin, original magnification X10).
|
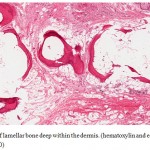 |
Figure 2: Rings of lamellar bone deep within the dermis. (hematoxylin and eosin, original magnification X20).
|
 |
Figure 3: Focal osteoclastic activity at the internal margins of the bone. (hematoxylin and eosin, original magnification X40).
|
Discussion
Many interesting changes may be seen in nevi, such as amyloid, nodular myxoid changes, folliculitis, and granular cell changes. 5 6 7 Bone formation in nevi is another unusual finding that is reported to range from 20% to 60% of all skin lesions with ossifications in large series studies. 2 8 4 It has been called osteo-nevus of Nanta who reported it in detail in 1911, although Heidingsfeld was the first to describe a melanocytic nevus with ossification in 1908. 9 10 Majority of cases of nevus of Nanta involve the skin of the face or head with unequivocal female predominance. 4 2
The pathogensis of the ossification within the nevi is not precisely understood. In 1977, Burgdorf and Nasemann have proposed two mechanisms by which cutaneous ossification may occur: 1) primitive mesenchymal cells transformation into osteoblasts that produce bone or 2) metaplastic transformation of other undetermined dermal cells that’s stimulated by the appropriate cellular milieu. 11 Bone formation in nevi is a form of heterotopic ossification which might be attributed to several factors and the transformation of primitive cells of mesenchymal origin into osteogenic cells is thought to be the pathogenesis of such process. 12 Three factors have been proposed for ossification of soft tissues to occur: osteogenic precursor cells, inducing agents, and a permissive environment. 13 In Conlin et al study, 13 of 15 cases of osteo- nevus occurred in female patients, so they suggested that a higher incidence in females may be related to estrogenic effect on osteoblasts. The association with folliculitis has been addressed in Moulin et al study, in which he studied 125 cases of nevus of Nanta, and observed that all nevi contained hair follicles. It has been proposed that folliculitis by trauma or neoplastic proliferation might induce dermal fibroblasts to differentiate into osteoblasts. 4 Interestingly, most of the lesions involve the face and facial skin get easily irritated by trauma or infection, rich in hair follicles and of more concern for cosmetic reasons. Among other factors, Transforming growth factor-B and connective tissue growth factor have been suggested as key players in ossification of nevus of Nanta. 14 Although there are several hypotheses, the exact pathogenesis is currently not fully understood and further studies are needed to test these hypotheses.
Although bone formation in melanocytic nevi is uncommon phenomena, none of the large series studies reported any malignant transformation of these lesions. There is only one report of malignant melanoma arising in osteo-nevus of Nanta. 15
In conclusion, this is a report of unusual case of osseous metaplasia within an intradermal melanocytic nevus, osteo-nevus of Nanta. Oral and Maxillofacial pathologist might receive skin biopsy from facial and perioral regions, therefore they should be aware of this rare entity. The possible pathogenesis hypotheses have been discussed briefly.
Acknowledgment
The author would like to thank Dr. Hessa Al Waily for referring the case.
References
- Rubin, A. Weedon’s skin pathology. (Churchill Livingstone Elsevier: [London], 2010).
- Conlin, P.A., Jimenez-Quintero, L.P. & Rapini, R.P. Osteomas of the skin revisited: a clinicopathologic review of 74 cases. Am J Dermatopathol 24, 479-483 (2002).
- Boyd, A.S. & King, L.E., Jr Basal cell carcinoma with ossification. J. Am. Acad. Dermatol. 38, 906-910 (1998).
- Moulin, G., Souquet, D. & Balme, B. [Pigmented nevus and cutaneous ossifications. Apropos of 125 cases of osteonevi]. Ann Dermatol Venereol 118, 199-204 (1991).
- MacDonald, D.M. & Black, M.M. Secondary localized cutaneous amyloidosis in melanocytic naevi. Br. J. Dermatol. 103, 553-556 (1980).
- Mehregan, D.R., Mehregan, D.A. & Mehregan, A.H. Nodular myxoid change in melanocytic nevi. A report of two cases. Am J Dermatopathol 18, 400-402 (1996).
- El-Gamal, H.M., Robinson-Bostom, L., Saddler, K.D., Pan, T. & Mihm, M.C. Compound melanocytic nevi with granular cell changes. J. Am. Acad. Dermatol. 50, 765-766 (2004).
- Sasaki, S., Mitsuhashi, Y. & Ito, Y. Osteo-nevus of Nanta: a case report and review of the Japanese literature. J. Dermatol 26, 183-188 (1999).
- Heidingsfeld, L.M. Osteoma cutis. Archiv für Dermatologie und Syphilis 92, 337-342 (1908).
- Nanta, M. Sur I’osteo-naevus. Ann Dermatol Syphil 2, 562
- Burgdorf, W. & Nasemann, T. Cutaneous osteomas: a clinical and histopathologic review. Arch Dermatol Res 260, 121-135 (1977).
- Urist, M.R., Nakagawa, M., Nakata, N. & Nogami, H. Experimental myositis ossificans: cartilage and bone formation in muscle in response to a diffusible bone matrix-derived morphogen. Arch. Pathol. Lab. Med. 102, 312-316 (1978).
- Chalmers, J., Gray, D.H. & Rush, J. Observations on the induction of bone in soft tissues. J Bone Joint Surg Br 57, 36-45 (1975).
- Keida, T., Hayashi, N., Kawakami, M. & Kawashima, M. Transforming growth factor beta and connective tissue growth factor are involved in the evolution of nevus of Nanta. J. Dermatol 32, 442-445 (2005).
- Culver, W. & Burgdorf, W.H. Malignant melanoma arising in a nevus of Nanta. J. Cutan. Pathol 20, 375-377 (1993).
Accepted on: 04 November 2011








![]()
![]()
