
Prescribing Patterns, Safety Outcomes, and Predictors of Adverse Events with Oral Hypoglycemic Agents in Type 2 Diabetes Mellitus Patients with Comorbidities: A Prospective Observational Study
 , Awanish Tiwari1, Mohd. Anas1, Gberme Alfred Gongbo1, Javed Akhtar Ansari1*and Parvez Saeed2
, Awanish Tiwari1, Mohd. Anas1, Gberme Alfred Gongbo1, Javed Akhtar Ansari1*and Parvez Saeed2 1Department of Pharmacy Practice, Faculty of Pharmacy, Integral University, Lucknow, India.
2Department of General Medicine, Faculty of Medicine and Health Sciences, Integral University, Lucknow, India.
Corresponding author Email: javed.ansari47@gmail.com
DOI : http://dx.doi.org/10.13005/bbra/3467
Download this article as:
![]()
This prospective observational study on Type 2 diabetes mellitus (T2DM) often occurs with multiple comorbidities, predisposing patients to polypharmacy and a higher risk of adverse drug reactions (ADRs) and drug–drug interactions (DDIs). This study included 105 T2DM patients receiving oral hypoglycemic agents (OHAs) in a tertiary care hospital over six months. Prescriptions were reviewed for utilization patterns, brand versus generic use, and extent of polypharmacy. ADRs were assessed using Naranjo, Hartwig, and Schumock–Thornton scales, and DDIs were identified through the Micromedex database. The mean patient age was 56.8 ± 10.2 years, and females comprised 54.3%. Each prescription contained an average of 10.9 ± 2.3 drugs, with 97.9% prescribed by brand name. Metformin alone (27.6%) and metformin–glimepiride (39.0%) were most common. ADRs occurred in 35.2% of patients, predominantly gastrointestinal (45.9%) and neurological (43.2%), with 14% preventable. Polypharmacy (OR = 2.13, p = 0.041) and hypertension (OR = 2.46, p = 0.029) significantly predicted ADRs. Thirty-five clinically relevant DDIs were detected, 60% classified as major, mainly involving aspirin–metformin and aspirin–glimepiride. The study highlights extensive polypharmacy, minimal generic prescribing, and substantial safety concerns, emphasizing the need for rational drug use and strengthened pharmacovigilance in diabetes care.
KEYWORDS:Adverse Drug Reactions; Drug–Drug Interactions; Oral Hypoglycemic Agents; Prescribing Patterns; Type 2 Diabetes Mellitus
Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by impaired insulin secretion, insulin resistance, or both, leading to persistent hyperglycemia and progressive microvascular and macrovascular complications.1 Globally, the burden of type 2 diabetes mellitus (T2DM) continues to rise, with India emerging as one of the epicenters of this epidemic.2 Patients with T2DM frequently present with multiple comorbidities, such as hypertension, cardiovascular diseases, and infections, which demand complex pharmacotherapy and prolonged treatment durations.3
Oral hypoglycemic agents (OHAs) remain the mainstay of T2DM management and encompass various classes, including biguanides, sulfonylureas, dipeptidyl peptidase-4 (DPP-4) inhibitors, thiazolidinediones, sodium-glucose cotransporter-2 (SGLT2) inhibitors, and alpha-glucosidase inhibitors. While these agents are effective in reducing glycosylated hemoglobin (HbA1c) and preventing long-term complications, their use is frequently linked to adverse drug reactions (ADRs) such as hypoglycemia, gastrointestinal disturbances, weight gain, edema, and, in rare instances, cardiovascular or renal complications.4,5 In elderly individuals and those with multiple comorbidities, these risks are magnified by polypharmacy, which increases the potential for drug–drug interactions (DDIs) and may compromise therapeutic outcomes.6,7
Pharmacovigilance studies have shown that adverse drug reactions (ADRs) significantly contribute to morbidity, hospitalizations, and healthcare expenditures, particularly in older adults with diabetes.8 Although awareness of ADRs in T2DM management has improved, there remains a scarcity of real-world Indian data exploring the interrelationship among comorbidities, polypharmacy, and prescribing practices.9,10 Furthermore, challenges such as inappropriate prescribing, limited use of generic medications, and inadequate monitoring continue to exacerbate safety concerns.11
Given these issues, a systematic evaluation of prescribing trends and safety outcomes associated with oral hypoglycaemic agents (OHAs) in patients with comorbidities is essential. Comprehensive assessment of adverse drug reactions (ADR) profiles—including causality, severity, and preventability—along with the identification of clinically relevant drug-drug interactions (DDIs), can help guide rational prescribing and strengthen patient safety measures. Accordingly, the present study aimed to evaluate the prescribing patterns and safety outcomes (ADRs and DDIs) of OHAs among T2DM patients with comorbidities in a tertiary care hospital in North India. By focusing on a high-risk population within a real-world clinical setting, this investigation seeks to address a critical evidence gap and provide insights for optimizing diabetes pharmacotherapy in resource-limited healthcare environments.
Materials and Methods
This study was a six-month prospective observational investigation conducted in the Department of General Medicine at a tertiary care teaching hospital in North India between September 2022 and March 2023. The primary objective was to evaluate the prescribing patterns of oral hypoglycemic agents (OHAs) and assess their safety profile in patients with type 2 diabetes mellitus (T2DM) presenting with one or more comorbidities.
The study population comprised adult patients aged 30 years and above, of either sex, who had a confirmed diagnosis of type 2 diabetes mellitus (T2DM) and were receiving at least one oral hypoglycemic agents (OHA) during hospitalization. Only those with at least one comorbid condition—such as hypertension, cardiovascular disease, or infectious illness—were eligible for inclusion. Patients with type 1 diabetes mellitus, pregnant or lactating women, individuals with severe cognitive impairment or an unconscious state, and those unable to provide follow-up information were excluded. Based on the prevalence of ADRs in T2DM reported in earlier Indian studies, a minimum sample size of 105 patients was calculated using a single-proportion formula at a 95% confidence interval and a 9% margin of error.
Ethical clearance was obtained from the Institutional Ethics Committee prior to initiation of the study (IEC/IIMS&R/2023/51). Written informed consent was taken from all participants. The study was carried out in accordance with the ethical principles outlined in the Declaration of Helsinki (2008 revision).
A structured case record form was designed to collect demographic information, medical history, comorbidities, laboratory parameters, and detailed prescribing data, including drug name, formulation, dose, frequency, and whether the medication was prescribed by brand or generic name. The total number of drugs per prescription was recorded to evaluate the extent of polypharmacy.
All suspected adverse drug reactions (ADRs) were initially documented by treating physicians and later verified by the research team. Causality was determined using the Naranjo algorithm.12 The severity of ADRs was classified using the Hartwig and Siegel Severity Assessment Scale, and preventability was assessed using the Schumock and Thornton criteria. Potential drug–drug interactions (DDIs) were identified and categorized through the Merative Micromedex® database, with confirmation from Stockley’s Drug Interactions reference text.13 DDIs were classified as major, moderate, or minor, and their clinical implications—particularly hypoglycemia, hyperglycemia, or lactic acidosis—were recorded.
All collected data were entered into Microsoft Excel and analyzed using IBM SPSS Statistics version 26.0 (Trial Version, Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation, while categorical variables were presented as frequencies and percentages. Statistical comparisons were performed using the Chi-square or Fisher’s exact test for categorical data and the Student’s t-test or one-way ANOVA for continuous variables. To identify independent predictors of ADR occurrence, multivariate logistic regression analysis was applied, incorporating age, sex, number of comorbidities, and degree of polypharmacy as covariates. A p-value of less than 0.05 was considered statistically significant.
The following statistical tests were employed: Chi-square test to compare ADR incidence across age, gender, therapy type, and comorbidities; Fisher’s exact test for small cell counts (<5, e.g., ADRs with DPP-4 inhibitors); t-test or ANOVA to compare the mean number of drugs between ADR and non-ADR groups; and logistic regression to identify predictors such as polypharmacy and hypertension.
Results
Patient Demographics
A total of 105 patients with type 2 diabetes mellitus (T2DM) receiving oral hypoglycemic agents (OHAs) were enrolled in the study. The mean age of the cohort was 56.8 ± 10.2 years, with the majority belonging to the >50 years age group (54.3%), followed by 41–50 years (27.6%) and 30–40 years (18.1%). Females accounted for 54.3% (n = 57), while males comprised 45.7% (n = 48).
Adverse drug reactions (ADRs) were significantly more frequent in patients aged >50 years compared with those ≤50 years (67.6% vs. 32.4%; χ² = 6.21, p = 0.045). A higher incidence of ADRs was also observed among male patients (70.3%) than females (29.7%) (χ² = 4.97, p = 0.026).
Table 1: Age- and gender-wise distribution of T2DM patients on OHAs
| Age group (years) | Male (n) | Female (n) | Total (n) | Percentage (%) |
| 30–40 | 5 | 14 | 19 | 18.1 |
| 41–50 | 12 | 17 | 29 | 27.6 |
| >50 | 31 | 26 | 57 | 54.3 |
| Total | 48 | 57 | 105 | 100 |
Prescribing Patterns
Across the 105 prescriptions analyzed, a total of 1,150 drugs were prescribed, yielding a mean of 10.9 ± 2.3 medications per patient. The majority (97.9%) were prescribed by brand name, while only 2.1% were issued generically. Of the total medications, 127 (11.0%) were oral hypoglycemic agents.
Patients with polypharmacy (>10 drugs) exhibited a significantly higher incidence of ADRs compared with those receiving ≤10 drugs (42.6% vs. 20.6%; χ² = 5.33, p = 0.021).
Table 2: Prescription characteristics among T2DM patients.
| Parameter | Value |
| Total prescriptions analyzed | 105 |
| Total number of drugs prescribed | 1,150 |
| Average number of drugs per prescription | 10.9 ± 2.3 |
| Drugs prescribed by brand name | 1,126 (97.9%) |
| Drugs prescribed by generic name | 24 (2.1%) |
| OHAs prescribed | 127 (11.0% of all drugs) |
Utilization of Oral Hypoglycemic Agents
Monotherapy was observed in 38.0% of patients, with metformin being the most common single agent (27.6%), followed by glimepiride (9.5%) and DPP-4 inhibitors (0.9%). Combination therapy was more frequent (61.9%), with metformin–glimepiride combinations accounting for 39.0%. Patients on combination therapy showed a higher incidence of ADRs than those on monotherapy (40.9% vs. 23.1%; χ² = 4.02, p = 0.045).
Table 3: Utilization patterns of OHAs among T2DM patients.
| Therapy type | Drugs Prescribed | n | % |
| Monotherapy | Metformin | 29 | 27.6 |
| Glimepiride | 10 | 9.5 | |
| DPP-4 inhibitors | 1 | 0.9 | |
| Combination therapy | Metformin + Glimepiride | 41 | 39.0 |
| Metformin + Pioglitazone + Glimepiride | 2 | 1.9 | |
| Voglibose + Metformin | 2 | 1.9 | |
| Vildagliptin + Metformin + Glimepiride | 3 | 2.9 | |
| Teneligliptin + Metformin | 3 | 2.9 | |
| Other combinations | 14 | 13.3 |
Adverse Drug Reactions (ADRs)
A total of 37 adverse drug reactions (ADRs) were recorded, corresponding to an overall incidence of 35.2%. The majority occurred among patients aged >50 years (67.6%), followed by those aged 41–50 years (24.3%) and 30–40 years (8.1%). Males experienced more ADRs than females (70.3% vs. 29.7%).
Table 4: ADR distribution by age group.
| Age group | n (ADRs) | % |
| 30–40 | 3 | 8.1 |
| 41–50 | 9 | 24.3 |
| >50 | 25 | 67.6 |
Table 5: ADR distribution by gender.
| Gender | n (ADRs) | % |
| Male | 26 | 70.3 |
| Female | 11 | 29.7 |
Gastrointestinal symptoms (45.9%) were the most frequent adverse drug reactions (ADRs), including decreased appetite, vomiting, bloating, and dyspepsia, predominantly linked to metformin. Neurological effects (43.2%), such as dizziness and headache, were primarily associated with sulfonylureas. Other reactions included diarrhea (2.7%) with DPP-4 inhibitors and skin rash (2.7%) with alpha-glucosidase inhibitors. Gender differences in ADRs may result from variations in body composition, hormonal levels, enzyme activity, drug metabolism, and immune response, with studies suggesting that females often tolerate certain drugs better than males due to hormonal and metabolic factors.
Table 6: ADRs by drug class and organ system.
| Drug class | Organ system affected | Common ADRs | n (ADRs) | % of total |
| Biguanides (Metformin) | Gastrointestinal, Neurological | Decreased appetite, vomiting, bloating, headache | 17 | 45.9 |
| Sulfonylureas (Glimepiride) | Neurological, Gastrointestinal | Dizziness, abdominal pain, constipation | 16 | 43.2 |
| DPP-4 inhibitors | Gastrointestinal | Diarrhea | 1 | 2.7 |
| Alpha-glucosidase inhibitors | Dermatological | Rash | 1 | 2.7 |
Causality assessment using the Naranjo algorithm classified 30 adverse drug reactions (ADRs) (81%) as “probable” and 7 (19%) as “possible.” According to Hartwig’s severity scale, 59% were mild, 35% moderate, and 6% severe. Using Schumock and Thornton criteria, 14% were definitely preventable, 49% probably preventable, and 37% not preventable.
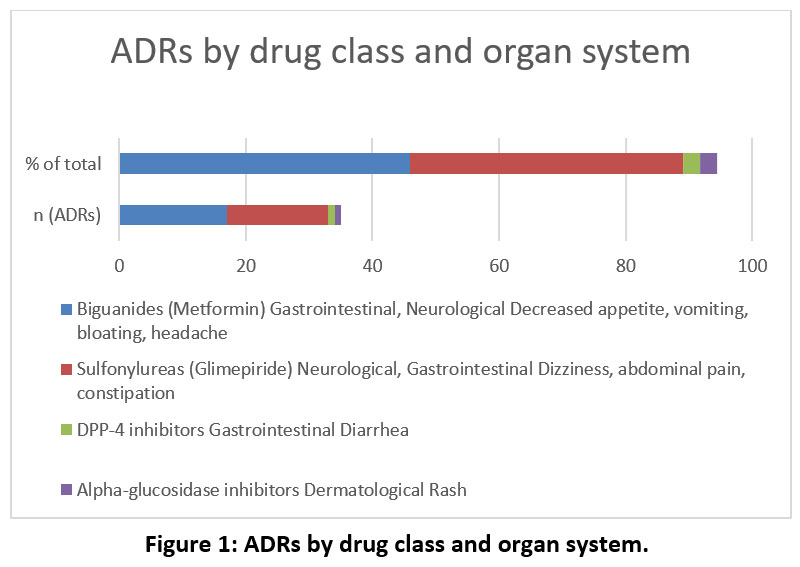 |
Figure 1: ADRs by drug class and organ system. |
Table 7: Causality, severity, and preventability of ADRs.
| Scale | Categories |
| Naranjo causality | Probable: 30 (81%), Possible: 7 (19%) |
| Hartwig severity | Mild: 22 (59%), Moderate: 13 (35%), Severe: 2 (6%) |
| Schumock & Thornton preventability | Definitely preventable: 5 (14%), Probably preventable: 18 (49%), Not preventable: 14 (37%) |
Multivariate logistic regression identified polypharmacy (>10 drugs) (OR = 2.13, 95% CI: 1.02–4.46, p = 0.041) and hypertension (OR = 2.46, 95% CI: 1.11–5.44, p = 0.029) as independent predictors of ADRs.
Comorbidities
A total of 62 comorbidities were recorded. Hypertension was the most common (41.9%), followed by respiratory tract infections (14.5%), urinary tract infections (3.2%), and other conditions (40.3%). ADRs occurred more frequently in patients with hypertension than in those without (46.2% vs. 28.1%; χ² = 4.11, p = 0.043).
Table 8: Distribution of comorbidities among T2DM patients.
| Comorbidity | n | % of total |
| Hypertension | 26 | 41.9 |
| Respiratory infection | 9 | 14.5 |
| Urinary tract infection | 2 | 3.2 |
| Other | 25 | 40.3 |
Drug–Drug Interactions (DDIs)
Thirty-five clinically significant drug-drug interactions (DDIs) were detected, of which 21 (60%) were major and 14 (40%) moderate. The most frequent major interactions involved aspirin + metformin (10 cases) and aspirin + glimepiride (5 cases), both associated with increased hypoglycemia risk. Levofloxacin–metformin (3 cases) and glimepiride–levofloxacin (1 case) were also identified as major interactions. Moderate interactions included furosemide + glimepiride (7 cases) and glimepiride + β-blockers (4 cases). Patients with two or more comorbidities exhibited a significantly higher frequency of DDIs compared to those with fewer comorbidities (41.7% vs. 19.5%; χ² = 5.72, p = 0.017).
Table 9: Common drug–drug interactions observed.
| Drug combination | Severity | Clinical outcome | Frequency (n) |
| Aspirin + Metformin | Major | Increased risk of hypoglycemia | 10 |
| Aspirin + Glimepiride | Major | Increased risk of hypoglycemia | 5 |
| Levofloxacin + Metformin | Major | Altered glucose control | 3 |
| Glimepiride + Levofloxacin | Major | Altered glucose control | 1 |
| Furosemide + Glimepiride | Moderate | Hyperglycemia, ↑ insulin requirement | 7 |
| Glimepiride + β-blocker | Moderate | Masked hypoglycemia symptoms | 4 |
| Other combinations | Moderate | Various | 5 |
Discussion
The present study provides a comprehensive evaluation of prescribing patterns, adverse drug reactions (ADRs), and drug–drug interactions (DDIs) associated with oral hypoglycemic agents (OHAs) among patients with type 2 diabetes mellitus (T2DM) and comorbidities in a tertiary care teaching hospital. Several key observations emerged: high rates of polypharmacy, predominant use of brand-name prescriptions, frequent use of metformin–glimepiride combinations, and a substantial burden of ADRs and clinically relevant DDIs.
The average number of drugs prescribed per patient (10.9 ± 2.3) was notably higher than that reported in comparable Indian studies (6–8 drugs per prescription).14,15 This reflects the therapeutic complexity of managing T2DM alongside comorbid conditions such as hypertension and infections. However, it also underscores a concerning trend of irrational polypharmacy, which increases the risk of ADRs and drug interactions. In the present study, polypharmacy was independently associated with higher ADR incidence, aligning with previous research linking excessive medication use to reduced adherence and greater adverse outcomes.16 Furthermore, the overwhelming preference for brand-name prescribing (97.9%) deviates from World Health Organization (WHO) recommendations promoting generic prescriptions, with implications for both treatment affordability and rational use.
Metformin remained the most frequently prescribed OHA, consistent with ADA/EASD guidelines recommending it as first-line therapy for T2DM.17 The metformin–glimepiride combination was the predominant regimen (39%), reflecting its widespread acceptance due to cost-effectiveness and synergistic efficacy in glycemic control. However, the limited use of newer agents, such as DPP-4 inhibitors (0.9% in monotherapy, 5.8% in combinations), contrasts with global prescribing trends favoring these drugs for patients with cardiovascular or renal comorbidities.18 This gap may be attributed to high cost, restricted availability, and prescriber familiarity with conventional agents in government and teaching hospitals, illustrating the disconnect between international recommendations and local practice patterns.
The overall ADR incidence of 35.2% is comparable to Indian pharmacovigilance reports (30–40%) but higher than data from Western cohorts (15–20%).19, 20 Gastrointestinal disturbances, predominantly linked to metformin, and neurological effects related to sulfonylureas were the most common. Although most ADRs were mild or moderate, approximately one-fifth were preventable, suggesting room for intervention through closer monitoring and patient education. Elderly patients, males, and those with hypertension or polypharmacy were particularly vulnerable—findings consistent with established risk factors in prior literature. 21
The Naranjo causality assessment identified most ADRs as “probable,” which supports the clinical attribution of adverse outcomes to OHAs. The detection of severe ADRs, though infrequent, underscores the need for proactive pharmacovigilance in high-risk individuals.
Hypertension was the most common comorbidity (41.9%) and independently associated with ADR occurrence. This finding emphasizes the therapeutic complexity of managing T2DM–hypertension coexistence, where multiple agents targeting different pathways can interact pharmacodynamically.
A total of 35 clinically significant drug–drug interactions (DDIs) were identified, with 60% categorized as major. The most frequent interactions—aspirin with metformin and aspirin with glimepiride—carry a high risk of hypoglycemia. These observations mirror previous Indian studies reporting similar drug–drug interactions (DDIs) profiles in patients receiving combined cardiovascular and antidiabetic therapy. Interactions involving fluoroquinolones, particularly levofloxacin, were also clinically important, as they may precipitate dysglycemia and lactic acidosis when combined with OHAs. The higher prevalence of drug–drug interactions (DDIs) among patients with multiple comorbidities highlights the urgent need for regular medication reviews and the integration of electronic interaction-checking systems into hospital prescribing workflows.
The findings of this study underscore three critical issues in diabetes management: excessive polypharmacy, predominant brand-name prescribing, and underuse of evidence-based newer OHAs. These factors collectively contribute to higher ADR rates, reduced medication adherence, and increased healthcare costs. Strengthening clinical pharmacy services, promoting prescription audits, and encouraging adherence to guideline-directed therapy can mitigate these problems. Routine involvement of clinical pharmacists in prescription review processes may help identify potential drug–drug interactions (DDIs), reduce preventable ADRs, and support rational medication use.
Promoting generic prescribing and pharmacist-led interventions can enhance treatment affordability, safety, and adherence in diabetes care. Integrating clinical pharmacists into routine prescription reviews may help identify drug–drug interactions, reduce preventable ADRs, and support rational medication use in alignment with national pharmacovigilance goals.
The strengths of this study include its prospective design, systematic evaluation of ADRs and drug–drug interactions (DDIs) using validated scales (Naranjo, Hartwig, Schumock, and Micromedex), and the use of multivariate analysis to identify independent predictors of ADRs.22 However, certain limitations should be acknowledged. The single-center setting may limit generalizability, and the six-month duration could underestimate long-term ADRs or cardiovascular outcomes. Additionally, causality assessments relied on clinical judgment rather than dechallenge–rechallenge verification. Future multicentric studies with longer follow-up and electronic prescribing surveillance are warranted to validate and expand these findings.
Although numerous studies have examined diabetes pharmacotherapy, few Indian investigations have comprehensively analyzed prescribing trends, ADR burden, and DDIs within the same patient cohort using multivariate modeling. By identifying polypharmacy and hypertension as independent predictors of ADRs and highlighting the prevalence of major DDIs in real-world practice, this study provides valuable evidence for safer and more rational diabetes management in resource-limited settings.
Conclusion and Directives
This study demonstrates that prescribing practices for type 2 diabetes mellitus in a tertiary care setting are characterized by extensive polypharmacy, predominant brand-name prescribing, and frequent use of metformin–glimepiride combinations. Although metformin remains the cornerstone of therapy in alignment with international guidelines, the limited use of newer oral hypoglycemic agents reflects a gap between evidence-based recommendations and real-world practice.
A high incidence of adverse drug reactions (35.2%) and clinically relevant drug–drug interactions (33.3%) was observed, with polypharmacy and hypertension emerging as significant predictors of ADRs. These findings highlight the need for rational prescribing, regular medication reviews, and strengthened pharmacovigilance systems to enhance treatment safety.
Integrating pharmacist-led interventions, structured prescription audits, and electronic decision-support tools can reduce preventable ADRs and improve therapeutic outcomes. From a policy perspective, promoting generic prescribing and adherence to WHO and ADA/EASD guidelines can improve both affordability and safety in diabetes management.
Future research should focus on multicentric, longitudinal studies that evaluate long-term safety outcomes and incorporate pharmacoepidemiological and pharmacogenomic data. Linking clinical outcomes with cost analyses may also help inform evidence-based healthcare policies in resource-constrained settings.
Acknowledgment
The authors would like to thank Hon. Chancellor, Pro-chancellor, and Vice-chancellor, Integral University, Dean, Faculty of Pharmacy, and Head, Department of Pharmacy, Integral University for providing the facility to complete this work. The Integral University has provided a manuscript communication number for further communication (IU/R&d/2024-MCN0002629).
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This article contains studies with human participants. The work was approved by the Institutional Ethics Committee, IIMS&R Integral University, Lucknow (IEC/IIMS&R/2023/51).
Informed Consent Statement
Written informed consent was obtained for the present study and that it conforms to the standards currently applied in the country of origin. The privacy rights of human subjects were observed.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from other sources
Not Applicable
Author’s Contributions
Indraj Kumar Yadav: Writing – Original Draft.
Awanish Tiwari: Data Collection
Anas: Data analysis.
Gberme Alfred Gongbo: Writing – Review & Editing.
Javed Akhtar Ansari: Visualization, Supervision, Project Administration.
Parvez Saeed: Conceptualization, Supervision.
Reference
- American Diabetes Association (ADA). Standards of medical care in diabetes—2023. Diabetes Care. 2023;46(Suppl 1):S1–S200. Available from: https://diabetes.org/newsroom/american-diabetes-association-2023-standards-care-diabetes-guide-for-prevention-diagnosis-treatment-people-living-with-diabetes
- Kshirsagar NA, Lihite RJ. Pharmacovigilance in India: Recent developments and future directions. Ther Adv Drug Saf. 2021; 12:20420986211002402. doi:10.1177/20420986211002402
- Naqvi SAH, Singh A, Yadav A, Ahmed J, Ahmad MA, Akhtar MS, et al. Drug utilization pattern and adverse drug reaction monitoring of antibiotics use in ear, nose, and throat infections at a tertiary care hospital, Lucknow, India. Indian J Health Care Med Pharm Pract. 2023;4(1):71–81. doi:10.22541/au.167925245.50477547/v1
CrossRef - Keezhipadathil J. Evaluation of suspected adverse drug reactions of oral anti-diabetic drugs in a tertiary care hospital for type II diabetes mellitus. Indian J Pharm Pract. 2019;12(2):82–87. doi:10.5530/ijopp.12.2.17
CrossRef - Shanthi M, Madhavrao C. Study of adverse drug reaction and causality assessment of antidiabetic drugs. Int J Basic Clin Pharmacol. 2019;8(1):56–61. doi:10.18203/2319-2003.ijbcp20185065
CrossRef - Basnet S, Paudel KR, Sah AK, Jha RK, Sah P, Adhikari S, et al. Prescribing pattern, polypharmacy and potentially inappropriate prescribing in hospitalized elderly patients: a retrospective study in a teaching hospital in Nepal. Int J Sci Rep. 2016;2(1):7–12. doi:10.18203/issn.2454-2156.IntJSciRep20160087
CrossRef - Goren Z, Demirkapu MJ, Acet GA, Cali S, Oglu MGI. Potential drug–drug interactions among prescriptions for elderly patients in primary health care. Turk J Med Sci. 2017;47(1):47–54. doi:10.3906/sag-1504-124
CrossRef - Fadare JO, Olamoyegun MA, Ajayi IO, et al. Polypharmacy and its determinants among patients with chronic diseases in primary care: a cross-sectional study. BMC Health Serv Res. 2021;21(1):534. doi:10.1186/s12913-021-06514-3
- Dominic A, Joseph J, Augustine RM, Begum R, Nanjwade BK. Study of drug use evaluation on oral antihyperglycemic agents in type 2 diabetes mellitus and their potential drug–drug interactions. World J Pharm Pharm Sci. 2016;5(7):1884–1896. doi:10.20959/wjpps20167-7261
- Ramaraju S, Dash S, Choudhary R. Prescribing pattern and implementation of clinical pharmacy services in patients with type 2 diabetes mellitus and its complications in a tertiary care hospital, Bangalore. World J Pharm Res. 2017;6(15):1295–1309. doi:10.20959/wjpr201715-9646
- Alam MS, Aqil M, Qadry SA, Kapur P, Pillai KK. Utilization pattern of oral hypoglycemic agents for diabetes mellitus type 2 patients attending out-patient department at a university hospital in New Delhi. Pharmacol Pharm. 2014;5(7):636–645. doi:10.4236/pp.2014.57073
CrossRef - Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. doi:10.1038/clpt.1981.154
CrossRef - Stockley IH. Stockley’s Drug Interactions. 6th ed. London, UK: Pharmaceutical Press; 2002. doi:10.1080/10915810490269663A
CrossRef - Sharma S, Bansal R, Gupta S. Evaluation of prescribing pattern in patients of type 2 diabetes mellitus: a hospital-based study. J Evol Med Dent Sci. 2019;8(18):1440–1445. doi:10.14260/jemds/2019/320
CrossRef - Kumar A, Sharma P, Mehta R. Prescribing patterns and adverse drug reactions in type 2 diabetes mellitus patients: an observational study. Int J Basic Clin Pharmacol. 2021;10(6):665–671. doi:10.18203/2319-2003.ijbcp20211815
- Alwhaibi M, Balkhi B, Alhawassi TM, Alkofide H, Aldemerdash T, Alshammari TM, et al. Polypharmacy among patients with diabetes: a cross-sectional study in a tertiary hospital in Saudi Arabia. BMJ Open. 2018;8(5):e020852. doi:10.1136/bmjopen-2017-020852
CrossRef - Davies MJ, Aroda VR, Collins BS, Gabbay RA, Green J, Maruthur NM, et al. Management of hyperglycemia in type 2 diabetes, 2022. Diabetes Care. 2022;45(11):2753–2786. doi:10.2337/dci22-0034
CrossRef - Buse JB, Wexler DJ, Tsapas A, Rossing P, Mingrone G, Mathieu C, et al. 2019 update to: management of hyperglycemia in type 2 diabetes, 2018. Diabetes Care. 2020;43(2):487–493. doi:10.2337/dci19-0066
CrossRef - Pharmacovigilance Programme of India (PvPI). National Coordinating Centre–PvPI Annual Report 2020–21. Ghaziabad: Indian Pharmacopoeia Commission; 2021. Available from: https://www.ipc.gov.in/images/Annual_Report_2022_.pdf
- Alomar MJ, Alshammari TM, Aljadhey H, et al. A review of adverse drug reactions and reporting practices. Saudi Pharm J. 2020;28(7):983-993. doi:10.1016/j.jsps.2020.06.002
CrossRef - Kalra S, Gupta Y, Unnikrishnan AG. Preventing hypoglycemia: international and Indian perspectives. Indian J Endocrinol Metab. 2019;23(2):173–182. doi: 10.4103/ijem.IJEM_604_18
- Mishra P, Pal A, Hazra A, Das A. Drug–drug interactions in prescriptions for elderly: a multicentric study in India. Drugs Ther Perspect. 2020;36(2):82–90. doi:10.1007/s40267-019-00687-5
Accepted on: 25-11-2025
Second Review by: Dr. Karveer Aghade
Final Approval by: Dr. Eugene A. Silow








