
Prevalence and Risk Factors of Hepatitis B among Blood Donors in Al-Najaf Governorate
 , , Alaa Abdulhussein Rasool4 and Hashim Ali Abdualmeer Al-sherees5*
, , Alaa Abdulhussein Rasool4 and Hashim Ali Abdualmeer Al-sherees5* 1 Department of Microbiology. Main blood bank in AL-Najaf governorate/Iraq.
2Faculty of Chemistry University of Kashan/Iran
3Faculty of Science Kufa University/ Iraq.
4 Department of Microbiology, Najaf Health department/Iraq.
5 Department of Microbiology / faculty of Medicine / University of Kufa/Iraq.
Corresponding Author E-mail : hashimaa49@yahoo.com
DOI : http://dx.doi.org/10.13005/bbra/2878
Download this article as:
![]()
Hepatitis B virus (HBV) infection is a global problem. When the virus replicates in the hepatocytes, the liver functions will be impaired and the infection will spread throughout the liver. Blood and blood products contain HBV, and therefore the virus could be transmitted via blood transfusion. The aim of this study was to investigate the prevalence of viral hepatitis B (HBsAg and anti-HBc antibody) among the blood donors of the main blood bank in AL-Najaf governorate (central Iraq). We also analyzed some factors which may be associated with HBV infection. To do this, a total of 16273 blood samples were collected from voluntary donors from (20/5/2016) to (12/12/2016). The presence of HBV was tested by enzyme-linked immunosorbent assay (ELISA) for HBsAg and anti-HBc antibody. The samples were also analyzed in part for age range, gender, profession, liver enzymes and blood characterization. Our results showed that 41 individuals were chronically infected with HBV, one of them was female. Most of the infected patients were aged between 28-37 years old (47.6%). It is showed that HBV infected people have significantly higher levels of Serum Glutamic-Oxaloacetic Transaminase (SGOT) and Serum glutamic pyruvic transaminase (SGPT) compared with the control (P < 0.001 and P < 0.011 respectively). The increased levels were also observed for lymphocytes and platelets (P <0.055 and P <0.429 respectively). The results also showed that the virus is more distributed between drivers (33.3%).
KEYWORDS:Age Ranges; ALT; AST; Hepatitis B Virus; Blood Groups; Profession
Introduction
Hepatitis B virus (HBV) infection is a global problem. Two billion people were infected by hepatitis B virus and more than 360 million individuals suffer from chronic HBV infection. About 600,000 people die from hepatitis infection or the virus associated liver tumors called Hepatocellular Carcinoma (HCC). [1].
In Africa, more than fifty million people are chronically infected with hepatitis B, with about 25% risk of mortality. The rate of hepatitis B carriers in Africa (Sub-Sahara) is about 9%-20% [2]. The prevalence rate of the disease is about 4.8% to 21% in Ghana [3]. The causative agent of hepatitis B is an enveloped virus with Single Strand DNA (ssDNA) genome [4, 5]. When the virus replicates in the hepatocytes, the liver functions will be impaired and the infection will spread throughout the liver [6, 7]. Liver and hepatitis harm have increased as a consequence of the immune response against the virus in the liver cells [8].
Blood, blood products and body fluids such as vaginal secretions contain hepatitis B virus, and also the saliva of active carriers contains low concentrations of the virus [9]. The average incubation period of HBV is 90 days from the time of exposure to the onset of the symptoms but may vary from six weeks to six months [10].
The HBV transmission through blood and its products is a major health concern, especially in developing countries, where preparing the safe blood is still a primary challenge [11, 12]. The rate of viral hepatitis B infection is proportional to the rate of blood Transfusion Transmitted Hepatitis B Virus (TTHBV). The screening of the blood and its products prevents the transmission of infectious diseases that sometimes may not be cured. The only way to prevent the transmission of such diseases is to use more sensitive methods to examine the blood before transfusion [11, 12].
Materials and Methods
The diagnostic and research kits are listed in table 1 below.
Table 1: Kits that used by current study.
| No. | Kits | Manufacture | Origin |
| 1 | HBsAg | Bio kit | Spanish |
| 2 | Anti-HBc total | Bio kit | Spanish |
| 3 | HBsAg Ultra Vidas kit | Bio Merieux | France |
| 4 | GOT/AST-P III | Fujifilm | Japan |
| 5 | GPT/ALT-P III | Fujifilm | Japan |
Equipment and Materials
Table 2: The Equipment used by current study
| No. | Equipment and Instruments | Manufacturer | Origin |
| 1 | ELISA washer ELx50 | Bio Tek | USA |
| 2 | ELISA reader ELx 800 | Bio Tek | USA |
| 3 | ELISA printer Epson LQ 300+II | Bio Tek | USA |
| 4 | Incubator | Memmert | Germany |
| 5 | Refrigerator | DAIREI | USA |
| 6 | Centrifuge | Hettich | Germany |
| 7 | Timer with alarm | Rhythm | China |
| 8 | Micropipette 10-100 | Eppendorf | Germany |
| 9 | Hematology Analyzer | Diagon D-Cell 60 | Hungary |
| 10 | Vidas and Mini vidas | Biomerieux | France |
| 11 | FUJIFILM-Dry chemo | FUJIFILM | Japan |
Study Design
In brief, samples were collected from all the donors in addition to 20 apparently healthy controls. All the samples were typed for blood groups and tested by ELISA for HBsAg and anti-HBc antibody. Those who were diagnosed as infected by ELIZA as well as 10% of randomly selected samples with negative results were confirmed by ELFA. Then blood and liver factors were tested on patients and 20 healthy controls. After examining ELISA and VIDS, all samples were examined with tests for GOT, GPT enzymes, complete blood counts, and lymphocytes, as shown in Figure (1). Samples were collected from 16273 voluntary donors from (20/5/2016) to (12/12/2016). The presence of HBV was tested by enzyme-linked immunosorbent assay (ELISA) for HBsAg and anti-HBc antibody.
Methods
Diagnosis of HBsAg and Anti- HBc by ELISA–III
The detection of HBsAg anti-HBc was done by the use of the third generation of ELISA, technique using HBsAg and anti-HBc ELISA from BIO KIT (Spanish) and the assay was performed according to manufacturer ′s instructions.
Confirmatory of HBsAg by VIDAS (Mini VIDAS)
The confirmation of HBsAg was done by using VIDAS the assay was performed according to manufacturer ′s instructions. VIDAS HBsAg Ultra (HBs) is an automated qualitative test, the kit HBsAg Ultra from Biomerieux.
Results
Clinical Samples Distribution
A total of 16273 blood were collected in the main blood bank of AL-Najaf governorate. The mean age of the donors is 38.5 ±5.09 years (range: 18–59). All the samples were examined for the presence of HBsAg and anti-HBc antibody. The results are shown in the Table (3).
Table (3) Numbers of HBV positive according to the markers of HBV.
| No. of Donors | No. of HBsAg+ anti-HBc positive | No. of only HBsAg positive | No. of only anti-HBc positive | Total |
| 16273 | 42 (0.26 %) | 8 (0.05 %) | 278 (1.7 %) | 328 (2.01%) |
Our results showed that 42 people were HBsAg and anti-HBc positive (0.26%) and 41 out of them (97.6%) was male and the remaining one (2.4%) was female. It was also found that 278 individuals (1.7%) were only positive for anti-HBc antibody and eight individuals (0.05%) were positive for just HBsAg. All the donors were volunteers.
The prevalence of HBV exposure in Al-Najaf governorate was 2.01%, which 0.26% of them had an active infection. Eight individuals were only HBsAg positive means that they were at the beginning of HBV infection. Therefore, the incidence rate of HBV is 0.05%. The only anti-HBc antibody positivity indicating previous exposure that might be improved was seen in 278 people. Studies in the Middle East showed that the prevalence of HBsAg ranges from 4% to 5% in Iraq [13]. The present study shows the lower rate of this infection in Najaf city.
Gender of Donors
The classification of the data based gender in each age range group is shown in Table (4). The only notable fact of these tables is that the infection is less prevalent in women. But this could be a misinterpretation because the number of female participants are too small.
Table 4: The classification of samples by age and gender
| Age of Groups | No. of donors of males | No. of donors of females | Percent |
| 18-27 yr. | 3178 (19.5%) | 21 (0.13%) | 19.63 % |
| 28-37 yr. | 7623 (46.9%) | 26 (0.16%) | 47.06 % |
| 38-47 yr. | 1595 (9.8%) | 15 (0.09%) | 9.89 % |
| 48-57 yr. | 3426 (21.05%) | 9 (0.06%) | 21.11 % |
| 58 and more | 378 (2.3%) | 2 (0.01%) | 2.31 % |
| TOTAL | 16200 (99.55%) | 73 (0.45%) | 16273 (100%) |
Table 5: The classification of HBsAg and anti-HBc positive patients based on gender
| Gender | No. of Patients | Percent % |
| ⃰ Males | 41 | 97.62 % |
| Females | 1 | 2.38 % |
| Total | 42 | 100 % |
| Test | 4.25 Sign Males *P < 0.05 | |
*Statistically significant P value < 0.05
Profession of Patients
The results in chart (1) indicate the drivers can be infected by the virus more than the other professions significantly.
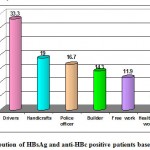 |
Chart 1: Distribution of HBsAg and anti-HBc positive patients based on profession. |
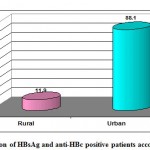 |
Chart 2: Distribution of HBsAg and anti-HBc positive patients according to residency |
Complete Blood Counts (CBC) of Patients
The blood factors collectively called CBC were analyzed for the patients and controls Tables (6).
Table 6: The classification of HBV patients and healthy control according to CBC
| RESULT | N. of Control | Percent % | N. of Patients | Percent% | T test P< 0.05 | |
| WBC | Normal | 11 | 55 | 19 | 45.2 | 3.2 |
| Low | 1 | 5 | 0 | 0 | 2.3 | |
| High | 8 | 40 | 23 | 54.2 | 4.3 | |
| HB | Normal | 10 | 50 | 39 | 92.9 | 6.6 |
| Low | 0 | 0 | 0 | 0 | NON | |
| High | 10 | 50 | 3 | 7.1 | 8.1 | |
| RBC | Normal | 6 | 30 | 31 | 73.8 | 7.8 |
| Low | 0 | 0 | 0 | 0 | NON | |
| High | 14 | 70 | 11 | 26.2 | 7.6 | |
| PLT | Normal | 17 | 85 | 32 | 76.2 | 3.3 |
| Low | 0 | 0 | 2 | 4.8 | 2.5 | |
| High | 3 | 15 | 8 | 19 | 2.2 | |
| MCHC | Normal | 2 | 10 | 4 | 9.5 | NON |
| Low | 18 | 90 | 37 | 88.1 | NON | |
| High | 0 | 0 | 1 | 2.4 | NON | |
| TOATL | 20 | 100 | 42 | 100 | ||
*Statistically significant P value < 0.05.
Statistical Analysis
This study was a kind of Cross-sectional study. Statistical analysis was done by using statistical package for social sciences (SPSS) version 17. The ANOVA test was used for the purpose of testing the differences between the means of the different variables, and the T-test was used to evaluate the differences between two groups. The LSD (Least Significant Differences) was used to detected significant differences between parameters, and Z-test was also used. P values less than the 0.05 was considered as statistically significant [14].
Discussion
To do this, 16273 volunteers were enrolled and blood samples were collected and analyzed. It was found that 42 people (0.26%) were infected as indicated by positivity for HBsAg and anti-HBc Antibody. This is lower than the report from Sulaimania governorate (0.67 [14], and it was also lower when compared to the neighboring Arab countries Lebanese blood donors (0.6%) [15], and much lower than Abuja (Nigeria) 17.5% [16]. It was much lower compared to Omani blood donors where HBsAg was present in 2.8% of the donors. [17]. Also, it was lower in AL-Anbar governorate, (west of Iraq) that the prevalence of HBsAg among screened total blood donors 16125 was 1.25%. [18].
The prevalence of chronic HBV infection is higher in men than women and this may be because of the rarity of volunteer female participants in this study.
In the current study, the prevalence of HBV result (2.01%) was similar to that in Sulaimania, Kurdistan Region-Iraq in 2006, which showed that the prevalence of HBV was 2.3% [19]. Our results showed the frequency of 0.31 for HBsAg which is lower than the prevalence reported for adults in New Zealand which showed that the prevalence of HBsAg was 0.5% [20]. The prevalence of HBsAg in our samples was lower than the result of Shahrekord (a city located in the west of Iran). Results showed HBsAg positivity in 1.78%; It is also lower than Shiraz (South-west Iran) where HBsAg was detected in 1.07% of samples; and Ghazvin (west-central) with HBsAg positivity of 1.08%; and also lower than HBsAg positivity reported from Kashan (center) which was 0.5%; and much lower than Tehran (North-central) with HBsAg positivity 3.4% [21]. Also, it was much lower than the prevalence of HBV among blood donors in Kosovo is 4.2%. [22].
However, my result was lower than that of a study which was done in the western Brazilian Amazon, which included 2656 samples; 3.3% were positive for HBsAg [23]. In the current study, there was no significant relation of HBsAg positivity with all ages but only in age (28-37) P-value < 0.05, while in gender showed a relative significance P-value < 0.05; a result which is similar to that of Blakely T. et al study [24].
Based on profession the current study revealed a significant relation of HBsAg positivity with the drivers 14 (33.3%) where the X2 calculation reached to (13.6) which is greater than the value of X2 (11.07) at a level of significance (P < 0.05) table (6). While for the other jobs it was not significant. This result was compatible with results of a study (Hepatitis B Prevalence and Risk Factors in Blood donors in Ghazvin which revealed that unemployed people, drivers, and barbers in Iran are at high risk [21], the barbers are also a high-risk group for HBV infection in Turkey [25], and drivers are a high-risk group as shown in another study in Iran [21].
In the current study, the driving was proposed as a risk factor for HBV infection. This may be because the drivers may deal with sharp tools during repairing cars or may have a low level of education and therefore have risky behaviors or may have extramarital sexual contact.
Conclusions
The prevalence of HBV among blood donors in Najaf is 2.01%.
The ratio of infected male to infected female blood donors was approximately 97.62%: 2.38%.
The prevalence of HBV among blood donors in the urban area (88.1%) is higher than the rural (11.9) area.
The driving profession has the higher risk for HBV infection among other professions.
The age group with the highest frequency of viral hepatitis B in Najaf governorate is 28-37 years old.
The study showed significant differences between patient’s hepatitis B and control in SGOT and SGPT.
The study showed a linear relationship between SGOT and SGPT.
The current study showed a P-probability of less than 0.05 in lymphocytes among patients with hepatitis B and control.
References
- Colin W.; Edgar S., P.; Lyn S., F.; Anthony E., F., and Beth P. B. (2006): Hepatitis B Virus Infection: Epidemiology and Vaccination. Epidemiologic Reviews. 28(1): 112-125.
CrossRef - Kiire C.F. (1996) The Epidemiology and Prophylaxis of Hepatitis B in Sub-Saharan Africa: A View from Tropical and Subtropical Africa. Journal of Gastroenterology and Hepatology. 38(2): 5-12.
CrossRef - Ghana Immunization Programme (2010). Comprehensive Multiyear Plan (2010-2014) in line with Global Immunization Vision and Strategies: 10-45.
- Taylor M., Purcell R.H., and Farci P. (2013) Hepatitis D (Delta) Virus. In: Knipe, D.M. and Howley, P.M., Eds., Fields Virology, 6th Edition, Lippincott Williams & Wilkins, Philadelphia. Open Journal of Medical Microbiology:4 (1) (2014).
- Tong M.J., Hsu, Chang P.W., and Blatt L.M., (2011). Evaluation of Current Treatment Recommendations for Chronic Hepatitis B: A 2011 Update. Journal of Gastroenterology and Hepatology. 26: 829-835.
CrossRef - Adams D.H., and Hubscher S.G. (2006). Systemic Viral Infections and Collateral Damage in the Liver. American Journal of Pathology.168: 1057-1059.
CrossRef - Vinciguerra M., Mazzoccoli G., Piccol C., Tataranni T., Andriel A., and Pazienza V. (2013). Exploitation of Host Clock Gene Machinery by Hepatitis Viruses B and C. World Journal of Gastroenterology.19: 8902-8909.
CrossRef - Rehermann B., and Nascimbeni M., (2005). Immunology of Hepatitis B Virus and Hepatitis C Virus Infection. Nature Review. Immunology: (5) 215-229.
CrossRef - CDC (2010) Sexually Transmitted Diseases Treatment Guidline. A. Kimberly, Workowski, Berman Stuart. (2010): 59(12):1-110.
- Mast , E., Weinbaum C., M., Fiore A., E., Alter M., J., Bell B., P., Finelli B.P., Rodewald L., Douglas E.L., Janssen M., R.S. and Ward, J. (2005). A Comprehensive Immunization Strategy to Eliminate Transmission of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices Part 1: Immunization of Infants, Children, and Adolescents. Morbidity and Mortality Weekly Report. Recommendations and Reports. 54: 1-31.
- MOH-Ghana (2006). National Blood Policy for the Health Sector: 5-25.
- World Health Organization (2006). Blood Transfusion Safety, Geneva: Page 2.
- Qirbi N., and Hall AJ., (2001). Epidemiology of hepatitis B virus infection in the Middle East. Eastern Mediterranean Health Journal. 7:1034-1045.
- The Iraqi Postgraduate Medical Journal 11, supplement. (2012).
- Ramia S., Ramlawi F., Kanaan M., Klayme S., and Naman R. (2005): Frequency and significance of antibodies against hepatitis B core (anti-HBc) antigen as the only serological marker for hepatitis B infection in Lebanese blood donors. Epidemiology and Infection. 133: 695–699.
CrossRef - Agbesor N., Innocent 1; E.2., Amala Smart; Zaccheaus A. (2013): Jeremiah 3 International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064. Index Copernicus Value 6.14. Impact Factor (2015): 6.3917.
- Geraldine K., Adel, Intesar A., Jameel N., and Said H. (2006): Evidence of Occult Hepatitis B Virus Infection among Omani Blood Donors: A Preliminary Study. Medical Principles and Practice. 15:368–372.
CrossRef - Yassin H., Majid. (2016). Hepatitis B Surface Antigen Prevalence Among Screened Populations and Certain Risk Groups in AL-Anbar governorate, AL- Anbar Medical Journal. 13 (1): 14-19.
CrossRef - Mohammed O. Mohammed. (2006): Prevalence of Hepatitis-B and Hepatitis-C among Blood Donors in Sulaimania City. Journal of Zankoy Sulaimania, 9: Part A 115-24.
CrossRef - Blakely T1.; Salmond C., and Tobias M. (1998): Hepatitis B virus carrier prevalence in New Zealand: population estimates using the (1987) police and customs personnel survey. New Zealand Medical Journal. 111(1064):142-4.
- Doosti A., Amini- Bavil- Olyaee S., Tajbakhsh E., Adeli A., Mahboudi F. (2009): Prevalence of viral hepatitis and molecular analysis of HBV among voluntary blood donors in west Iran. New microbiological. 32: 193-198.
- HajrullahFejza and SkenderTelaku. (2009): Prevalence of HBV and HCV among blood donors in Kosovo. Virology Journal. 6:21.
CrossRef - Sebasteao V., Raymundo P. (2005): High prevalence of hepatitis B virus and hepatitis D virus in the Western Brazilian Amazon. Tropical Medicine and Hygiene. 73:808-814.
CrossRef - Bandaranayake, Salmond CE., Tobias MI. (1991): Occupational risk of hepatitis B for police and customs personnel. 134:1447-53.
CrossRef - Candan , Alagozlu H., Poyraz O., and Sumer H. (2002): Prevalence of hepatitis B and C virus infection in barbers in the Sivas region of Turkey. Occupational Medicine Journal (London). 52:31-4.
CrossRef
Accepted on: 04-12-2020
Second Review by: Vikas Kaushik
Final Approval by: Dr. Eugene A. Silow








![]()
![]()
