
Drug Repurposing in Oncology: Progress, Challenges, and Collaborative Pathways Toward Novel Cancer Therapies
 and Shibin Ramchandran2*
and Shibin Ramchandran2* 1Department of Pharmacognosy, Faculty of Medicine and Health Science, Tagore College of Pharmacy, Chengalpattu, Tamil Nadu, India.
2Morepen Proprietary Drug Research Pvt Ltd, Hyderabad., India.
Corresponding Author Email: rshibinpharma17@gmail.com
DOI : http://dx.doi.org/10.13005/bbra/3455
Download this article as:
![]()
Drug repurposing is the process of trying to identify new therapeutic uses for approved existing drugs, which opens opportunities for development timescale shortening as well as early‐stage safety de‐risking. This review narrates the recent developments and challenges to drug repurposing in oncology, including translation strategies. We emphasize clinical examples, such as metformin (based on several randomised trials), propranolol (premature epidemiological and phase II proof) and thalidomide (FDA‐approved for multiple myeloma). Repurposing has clear benefits but the reuse courses are difficult to realize because of lack of biomarkers, intellectual property barriers, regulatory issues and complicated trials designs. We also describe computational strategies, such as signature‐reversal strategies interrogating from the TCGA integrative genomic resources. We conclude by delineating regulatory, economic and collaborative mechanisms that must be in place to achieve translation. This review offers current perspectives for biotechnological and clinical oncology researchers, and suggests actionable recommendations to sustain future repurposing pipelines.
KEYWORDS:Drug repurposing; leukaemia; Novel cancer therapies oncology; Tumors
Introduction
In oncology, drug repurposing has become a promising translational strategy that provides a workable answer to the problems associated with conventional drug development, including exorbitant expenses, protracted timelines, and frequent failures.1 This method increases patient access to novel treatments and lessens the burden of side effects by utilizing already-approved medications with proven safety profiles to speed the transition from lab research to clinical application.2 In environments with limited resources, where access to innovative cancer treatments is still a constant obstacle, the importance of drug repurposing is especially evident.3 Drug repurposing in oncology has a number of drawbacks despite its potential. In order to using single-agent approaches, combination therapies are frequently required due to the complexity of cancer biology, which is characterized by heterogeneity and multidrug resistance.4 However, the requirement to manage drug interactions, coordinate dosing, and address various mechanisms of action complicates the design and implementation of clinical trials for combination regimens.3 The incorporation of repurposed medications into clinical practice is further impeded by regulatory and commercial obstacles, such as restricted patent protection and diminished financial incentives.5 Recent developments in computational biology, organoid technology, and high-throughput screening have started to address some of these issues by making it possible to more precisely identify and validate repurposed medications.6 Personalized therapy and the development of new anticancer agents from existing drug libraries are now supported by patient-derived tumor organoids and biomarker-driven approaches.7 Precision oncology’s reach has been expanded by the use of computational prediction tools and curated databases, which have improved the capacity to match patient tumor profiles with possible repurposed therapies.8 Converting encouraging preclinical results into solid clinical outcomes is a recurring problem in the field, especially in light of the requirement for carefully planned prospective studies and the incorporation of multi-omics data for patient stratification.9 The broad use of repurposed medications in oncology is still hampered by a lack of predictive biomarkers, regulatory barriers, and inadequate financial incentives.10
By showcasing noteworthy success stories and analyzing the field’s potential future directions, this review seeks to present a thorough overview of the state of drug repurposing in oncology today. In order to influence future research and clinical practice, we will examine the approaches and technologies that have recently fueled advancements, assess the obstacles that still exist, and suggest solutions.11
Scope of the article
The following review provides an overview of the piece looks into drug repurposing by using current biotechnological tools. It covers approaches such as genomic profiling, transcriptomic signature analysis, molecular pathway mapping, computational prediction platforms, and high-throughput screening technologies. These techniques play a key role in modern bioscience studies. They help spot new ways to use existing drugs for treating cancer. The review pulls in details on mechanisms of action, biomarker creation, and strategies for moving research to real-world use. The article aims to present scientific advances, existing challenges, and future directions with the purpose of improving therapeutic development and patient outcomes in oncology.
What is Drug Repurposing in the Oncology context?
Beginning with the early days of cancer chemotherapy, drug repurposing in oncology has a long and dynamic history. One of the pioneering discoveries in the field was the discovery that mustard gas, a chemical warfare agent, could cause tumor regression in skin cancers.12 This coincidental finding paved the way for later attempts to find novel therapeutic applications for already-existing substances. The approach grew over time to encompass not only off-patent, generic medications but also agents that were still under patent and even medications that had not worked for their initial purposes. A notable example of pharmaceutical innovation through repositioning is the conversion of tamoxifen, which was first created as a contraceptive, into a ground-breaking treatment for breast cancer.13 Drug repurposing gained popularity as a practical substitute for traditional drug development as its cost, complexity, and duration increased. Due to established safety and pharmacokinetic profiles, which eliminate the need for early-phase clinical trials, the procedure is typically quicker and less costly. Repurposing can cut timelines to about six years and costs to a fraction of traditional approaches, whereas developing new drugs can take over ten years and cost billions of dollar.14
Collaborative efforts between academia, industry, and non-profit groups have advanced the field; organizations like the Repurposing Drugs in Oncology Project and the National Center for Advancing Translational Sciences have made significant contributions. Despite these developments, issues with profit and intellectual property have remained obstacles, especially for off-patent medications, which is why independent and academic research is crucial to producing clinical evidence.15-16 Developments in artificial intelligence, computational biology, and genomics have influenced the evolution of drug repurposing strategies in oncology.17-18 These days, personalized oncogenomics programs use tumor genetic data to inform logical clinical judgments, allowing for the choice of unconventional therapeutic approaches. For example, the discovery of particular genetic changes in tumors has made it possible to repurpose medications like imatinib, which was first created to treat chronic myeloid leukemia, to treat gastrointestinal stromal tumors that have comparable mutations.19-20
The use of multidrug personalized approaches, which frequently combine repurposed agents with novel therapeutics to overcome resistance mechanisms, has been further spurred by the realization that tumor heterogeneity and clonal evolution are the main causes of therapy resistance and relapse.21-24
Drug repurposing has been transformed by computational and artificial intelligence (AI)-driven approaches that combine knowledge graphs, machine learning models, and automated literature searches to forecast drug-target interactions and suggest promising candidates.25-27 As demonstrated by the use of tools such as the Connectivity Map and The Cancer Genome Atlas, signature-based and sequence-based approaches, which use gene or protein expression patterns from omics data, have also made it easier to identify medications that can reverse disease-associated signatures. Even with these technological advancements, there are still difficulties in managing large genetic datasets, detecting and validating cancer driver mutations, and dealing with resistance brought on by continuous tumor evolution.28-29
Traditional drug development is fundamentally different from drug repurposing. High attrition rates, a significant financial investment that frequently exceeds $2 billion and spans more than ten years, as well as extensive preclinical and clinical studies are characteristics of the conventional pathway for oncology drugs.30-33 Repurposing, on the other hand, makes use of medications with proven pharmacokinetic, toxicity, and safety profiles, enabling quick clinical translation and a lower failure rate.34-37 Cost and accessibility are important factors in low-income environments, where this strategy can be especially helpful.38-39 Additionally, repurposed medications can be quickly used in combination therapies, providing patients with limited effective treatments or drug resistance with new options. The broad clinical use of repurposed medications in oncology is still limited, though, by financial and regulatory barriers as well as a lack of patent incentives.40-41 Drug repurposing in cancer treatment has a number of justifications. It is motivated by the pressing need for faster, less harmful, and more effective treatments, particularly given the limitations of existing therapies and the rising incidence of cancer.42-43 By utilizing off-target effects pertinent to cancer pathways, like kinase inhibition, repurposing can reveal novel mechanisms of action for already-approved medications, facilitate combination strategies to overcome resistance, and broaden the clinical pipeline.44 The possibility of cross-indication repurposing is further supported by the biological similarities between cancer and other illnesses, such as cardiovascular disorders.45
To find promising candidates for repurposing, systematic methods like gene expression profiling and connectivity mapping are being utilized more and more.46-47
In oncology, drug repurposing offers significant advantages. In settings with limited resources and for rare or neglected cancers, repurposed medications provide faster development timelines, lower costs, and better access to therapies.48-50 The strategy boosts patient reach, permits individualized care, and raises the possibility of regulatory approval. Additionally, it makes it easier to implement combination treatments that can improve effectiveness, stop metastases, alter the metabolism of cancer cells, and get past resistance mechanisms. The discovery of novel therapeutic targets and drug interactions has been further improved by the application of computational and experimental approaches, as well as AI and bioinformatics tools.51-52 Notwithstanding these benefits, there are still many obstacles to overcome in oncology drug repurposing. The development of universally effective treatments is complicated by the biological complexity and heterogeneity of cancer, and regulatory requirements that might not allow for combination strategies frequently hinder the design of clinical trials.53 Financial and regulatory obstacles further impede clinical adoption, and intellectual property restrictions and a lack of patent incentives diminish industry interest, especially for generic medications.54-55 Biases in retrospective research, restricted access to information on compounds that have been shelved, and the absence of centralized repositories for discontinued medications are further challenges. Technical constraints and data quality concerns also make it difficult to integrate big datasets with sophisticated computational tools.56-57 All things considered, drug repurposing in oncology has advanced from accidental discoveries to a complex, interdisciplinary strategy that capitalizes on developments in artificial intelligence, computational biology, and genomics. This approach has a lot of potential to increase the number of cancer treatment options available, speed up therapeutic development, and lower costs, but achieving its full potential will necessitate concerted efforts to remove financial, scientific, and regulatory obstacles.
Methods and Strategies for Drug Repurposing in the Treatment of Cancer
The integration of computational, experimental, and molecular approaches has changed the landscape of drug repurposing in oncology. Each of these approaches brings special strengths to the identification and validation of novel therapeutic opportunities for cancer patients. The field now uses a wide range of advanced in silico, high-throughput, and pathway-based techniques to speed up the conversion of current medications into new cancer indications, building on a history of fortuitous discoveries and practical clinical observations. In the current era of drug repurposing, computational and in silico screening techniques have become essential tools. These methods use artificial intelligence, systems biology, and bioinformatics to analyze large datasets, forecast drug-target interactions, and rank candidates for experimental validation. The methodical examination of molecular networks made possible by the application of knowledge graphs and machine learning algorithms reveals hitherto unknown links between medications and carcinogenic pathways. For instance, signature-based techniques look for substances that can reverse disease-associated transcriptional signatures by comparing the gene expression profiles of cancer cells with those produced by different medications. This has been made possible by resources like the Cancer Genome Atlas and the Connectivity Map, which offer extensive omics datasets that make it easier to find repurposing candidates based on pathway perturbation and molecular similarity. Prioritizing medications with good safety profiles and well-established pharmacokinetics is made possible by the combination of clinical and pharmacological data with these computational techniques.
Notwithstanding the potential of computational methods, strong experimental validation is necessary to convert in silico predictions into clinically useful outcomes. In this regard, high-throughput screening platforms have become essential because they allow for the quick evaluation of sizable drug libraries against a variety of cancer cell lines and patient-derived models. The impact of thousands of compounds on cell viability, proliferation, and apoptosis is assessed by these platforms using automated technologies, producing rich datasets that guide the selection of candidates for additional research. The resolution of these screens has been further improved by developments in transcriptomics and proteomics, which make it possible to identify medications that molecularly alter important oncogenic pathways. To guide the logical design of combination therapies, transcriptomic profiling, for example, can show how candidate drugs affect the expression of genes linked to tumor growth, metastasis, and resistance. By combining computational predictions with high-throughput screening data, a potent feedback loop is produced that improves the selection of repurposing candidates and speeds up their advancement through the preclinical pipeline.
Drug repurposing relies heavily on pathway analysis and molecular targets. The rational selection of medications that can modulate these pathways, either alone or in conjunction with other agents, has been made possible by the discovery of actionable genetic alterations and dysregulated signaling cascades. In order to guide the repurposing of medications that may have been developed for other indications but possess pertinent mechanisms of action, pathway-based approaches use knowledge of cancer biology to identify points of vulnerability within the tumor. For instance, imatinib, a medication initially created for chronic myeloid leukemia, was successfully repurposed for the treatment of this uncommon cancer after activating mutations in the KIT gene were found in gastrointestinal stromal tumors. Similarly, mTOR inhibitors, which were first approved for organ transplantation, are now being evaluated in oncology settings due to the discovery of aberrant PI3K/AKT/mTOR signaling in a variety of malignancies. These examples underscore the importance of integrating molecular profiling with pharmacological knowledge to expand the repertoire of available cancer therapies. DNA methylation and other epigenetic changes are important for both the pathophysiology of cancer and the effectiveness of treatment. Understanding the mechanisms behind drug sensitivity and resistance can be gained by analyzing the methylation patterns in important oncogenes and tumor suppressor genes. For example, promoters of tumor suppressor genes may become silenced due to hypermethylation, which promotes unchecked cell division and tumor growth. DNA methyltransferase inhibitors and other medications that reverse abnormal methylation have demonstrated promise in the treatment of hematologic malignancies and are being investigated for potential repurposing in solid tumors. A thorough grasp of the molecular landscape of cancer is made possible by the combination of methylomics data with transcriptomic and proteomic analyses. This knowledge informs the choice of medications that can improve therapeutic efficacy and restore normal epigenetic regulation.
Numerous noteworthy success stories in oncology drug repurposing have resulted from the convergence of computational, experimental, and molecular approaches. The potential of this approach to provide patients with few options with transformative therapies is demonstrated by the repositioning of thalidomide, which was first created as a sedative, for the treatment of multiple myeloma. In a similar vein, a number of clinical trials are examining the potential of metformin, a commonly prescribed antidiabetic medication, to suppress the metabolism of cancer cells and make tumors more susceptible to traditional treatments. These illustrations show how important it is to use current pharmacological understanding and practical clinical experience to accelerate the creation of novel cancer therapies. Notwithstanding these developments, there are still a number of obstacles to overcome in the application of medication repurposing techniques in oncology. Finding universally effective treatments is made more difficult by the biological complexity and heterogeneity of cancer as well as the dynamic nature of tumor evolution. The durability of response to repurposed drugs is frequently limited by resistance mechanisms that are fueled by genetic diversification and clonal selection. Clinical decision-making involving large-scale omics datasets necessitates interdisciplinary cooperation and advanced analytical tools. The broad use of repurposed medications in oncology practice is further limited by regulatory and financial obstacles, such as complicated approval procedures and limited patent incentives.
Ongoing efforts are concentrated on improving computational models, increasing high-throughput screening capabilities, and integrating multi-omics data to fully capture tumor biology in order to overcome these obstacles. Collaborative initiatives involving academia, industry, and regulatory agencies are essential to facilitate data sharing, standardize methodologies, and streamline the translation of promising candidates into clinical trials. The effectiveness and impact of drug repurposing initiatives will be further increased by the creation of centralized repositories for shelved and abandoned compounds as well as methodical approaches to data integration and analysis.
Future developments in artificial intelligence, systems biology, and precision medicine will propel the ongoing development of drug repurposing in oncology. Deep learning algorithms have the potential to predict patient-specific therapy responses and reveal new drug-disease associations when applied to multi-dimensional datasets. Real-world data from patient registries, pharmacovigilance databases, and electronic health records will be integrated to offer important insights into the effectiveness and safety of repurposed medications in various clinical contexts. In order to ensure that cutting-edge treatments reach the patients who need them the most, a concerted effort to overcome scientific, regulatory, and financial obstacles will ultimately be necessary to realize the full potential of drug repurposing in oncology. All things considered, oncology drug repurposing is a vibrant and quickly developing field supported by developments in molecular pathway analysis, high-throughput testing, and computational biology. By combining these methods, new therapeutic opportunities have been found and validated, giving cancer patients hope for better results. Even though there are still many obstacles to overcome, maximizing the effectiveness of this strategy in the fight against cancer will require ongoing improvement of repurposing tactics and the growth of cooperative networks.
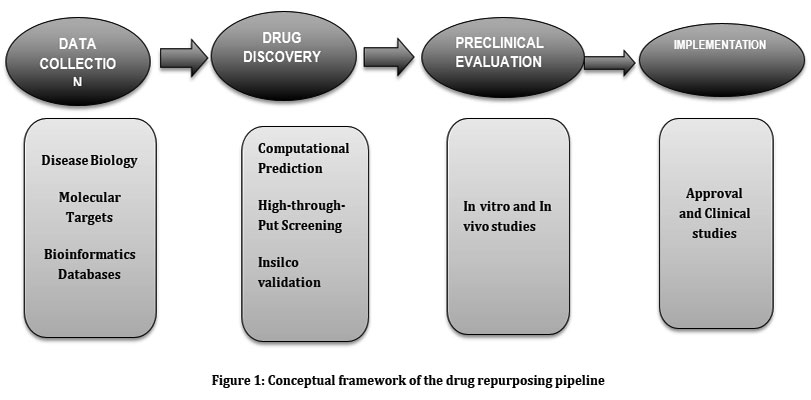 |
Figure 1: Conceptual framework of the drug repurposing pipeline |
Table 1: Summary of Computational Tools and Databases Used in Drug Repurposing
| Tool / Database | Type | Primary Function / Features | Applications in Drug Repurposing |
| Connectivity Map (CMap) – Broad Institute | Transcriptomic signature database | Compares drug-induced gene expression signatures with disease signatures | Identifies drugs that can reverse cancer-specific gene signatures; signature-based repurposing |
| TCGA (The Cancer Genome Atlas) | Genomic & transcriptomic database | Multi-omics cancer datasets (mutations, expression, methylation) | Mutation mapping, biomarker identification, molecular pathway-based drug matching |
| Drug Repurposing Hub (Broad Institute) | Curated compound database | Contains >6,000 compounds with mechanisms and clinical status | Source for screening repurposable compounds, mechanistic insights |
| PRISM Repurposing Resource | High-throughput drug screening database | Screens drugs across hundreds of barcoded cancer cell lines | Identifies compounds killing specific cancer genotypes |
| ReDO Database (Repurposing Drugs in Oncology Project) | Literature-based evidence database | Catalogs non-cancer drugs with anticancer potential | Supports evidence-based identification of repurposable drugs |
| PAD – Predictive Database for Drug Repurposing | Computational prediction platform | Integrates drug–gene and disease–gene networks | Ranks drug repurposing candidates using network-based prediction |
| CADDIE Platform | Drug–gene and gene–gene interaction modeling | Maps molecular networks and recommends repositionable drugs | Prioritizes drugs targeting cancer-specific pathways |
| Every Cure Platform | AI-integrated multi-dataset platform | Uses machine learning to merge EHR, PubMed, clinical trials data | Predicts new drug–disease associations efficiently |
| RepoDB | Approved vs. failed drug–indication dataset | Contains clinical outcomes of prior repurposing attempts | Helps validate computational predictions, improves trial selection |
| CURE ID | FDA & NCATS real-world reporting tool | Collects global clinical case reports on off-label drug use | Useful for identifying real-world success signals |
| DrugCentral | Comprehensive drug information system | Offers drug properties, targets, regulatory status | Supports early-stage computational filtering |
| DrugRepoBank | Repurposing-suitable compounds repository | Includes drugs with IP/market exclusivity information | Helps navigate commercial feasibility of repurposing |
| TCM Drug Repurposing Hub | Traditional medicine-focused compound database | Contains bioactive natural compounds and targets | Supports discovery of natural product-based repurposing |
| DESSCD – Dragon Exploration System | Literature mining system | Uses NLP to explore biomedical connections | Extracts mechanistic links for new repurposing hypotheses |
| Cancer Pharmacogenomics Network (CPN) | Clinical-genomic interaction database | Links genomic variants to drug responses | Identifies mutation-specific repurposing opportunities |
Oncology Drug Repurposing Success Stories
The integration of computational, experimental, and molecular strategies has allowed for the identification and validation of non-oncology drugs with demonstrated efficacy in cancer, leading to notable advancements in the field of drug repurposing in oncology. The ability of thousands of currently available medications, many of which were first created for non-cancer indications, to specifically target cancer cell lines has been systematically assessed through extensive screening efforts. For instance, a thorough investigation that screened more than 4,500 compounds found that almost 50 non-cancer medications could kill particular cancer cell types, frequently by means of hitherto unknown mechanisms. Notably, tepoxalin, an anti-inflammatory drug licensed for veterinary osteoarthritis, showed cytotoxicity against cancer cells that overexpressed MDR1, a protein linked to chemotherapy resistance. Similarly, vanadium-based compounds, originally created for diabetes, were effective against cancer cells expressing the sulfate transporter SLC26A2, and disulfiram, a medication for alcohol dependence, demonstrated efficacy in cell lines with mutations resulting in metallothionein depletion. These results lay the foundation for future clinical development and validation by highlighting the possibility of using the genomic characteristics of cancer cells as biomarkers to direct the selection of repurposed medications57 . In certain cancer subtypes, like mucoepidermoid carcinoma (MEC), the repurposing of non-oncology medications has also shown promise. While antiviral drugs like acyclovir and ganciclovir may stop tumor growth, preclinical models have shown that tocilizumab, an anti-IL-6R antibody used for arthritis, can improve the effectiveness of chemotherapy in MEC. Additional examples include valproate, an antiepileptic medication that functions as a histone deacetylase inhibitor, which reduces the survival of cancer stem cells, and curcumin, which targets important oncogenic pathways. By altering the STAT3 and NF-κB pathways, the antidiabetic medication metformin has demonstrated antiproliferative and anti-metastatic effects in MEC models. These results call for more clinical research because they demonstrate the potential of combining repurposed medications with conventional therapies to improve outcomes in cancers that are challenging to treat.58 Thalidomide, a medication with a complicated past, is one of the most noteworthy success stories in oncology drug repurposing. Thalidomide was first created as a sedative but subsequently discovered to have anti-inflammatory, immunomodulatory, and anti-angiogenic qualities. Though studies are frequently constrained by diverse patient populations and recruitment difficulties, thalidomide and similar drugs that target multiple cytokines and pathways have demonstrated clinical benefit in cancer-related cachexia. In multiple myeloma (MM), where it was the first immunomodulatory drug (IMiD) to increase survival, thalidomide had the most revolutionary effect. The median overall survival for younger MM patients has increased to more than ten years since the introduction of thalidomide, lenalidomide, and bortezomib. Though results are still worse than those in MM, thalidomide-based regimens have shown some improvement in survival in plasma cell leukemia, an uncommon and aggressive cancer.59- 61
The combination regimens of thalidomide and prednisone have demonstrated promising activity and favorable safety profiles in advanced castrate-resistant prostate cancer, where a significant percentage of patients have achieved notable reductions in prostate-specific antigen and a median overall survival of nearly 20 months. Thalidomide has also been evaluated in other malignancies. Thalidomide-based treatment, however, was linked to increased toxicity and failed to improve tumor response or survival in non-small cell lung cancer. Results for pancreatic and esophageal cancers have been conflicting; some studies have found poor tolerability and no benefit, while others have reported improvements in appetite and lean body mass at lower dosages. The significance of patient selection and disease context in repurposing strategies is underscored by these variable outcomes.62-64 Thalidomide is now understood to function as a molecular glue degrader, a class of medication that attracts target proteins to the cellular degradation machinery in order to cause their degradation. Additional targeted protein degraders have been developed as a result of this mode of action, broadening the therapeutic options for immune disorders and cancer.65
The potential anticancer effects of metformin, a medication that is frequently prescribed to treat diabetes, have also drawn a lot of attention. Metformin has been shown in preclinical and early-phase clinical trials to inhibit the proliferation of cancer cells, lower the risk of cancer, and improve prognoses for a variety of cancers. However, due to a lack of late-phase trials, especially in cancer patients who do not have diabetes, it is still unclear whether these findings will translate into clinical benefit. The effectiveness of metformin in cancer chemoprevention and treatment is presently being studied in many ongoing RCTs and clinical trials; however, the results have been conflicting thus far, with some studies indicating improved tumor response but no discernible benefit in survival. Metformin’s safety profile in diabetic populations is well-established; however, more research is needed to determine how it affects cancer patients who are not diabetic. Although meta-analyses and observational studies show that metformin use lowers the risk of developing cancer and improves survival rates, there is currently insufficient strong evidence to support its use as an adjuvant therapy for particular cancer types. It is anticipated that ongoing randomized controlled trials will elucidate its function and pinpoint the patient populations most likely to benefit.66- 79
Another repurposed medication with antitumor activity against over a dozen cancer types is propranolol, a non-selective beta-adrenergic receptor antagonist that was first prescribed for cardiovascular disorders. Its mechanisms include apoptosis induction, cell cycle disruption, tumor microenvironment modulation, and inhibition of cell proliferation. Propranolol has been demonstrated to improve apoptosis and decrease pro-proliferative markers in breast cancer, while it decreases proliferation indices like Ki-67 in gastric cancer. The use of propranolol has been associated in epidemiological studies with a decreased risk of a number of cancers, including esophageal, gastric, colon, prostate, and head and neck cancers. There is especially compelling evidence for hepatocellular carcinoma. Additionally, by downregulating prometastatic factors and the epithelial-mesenchymal transition, propranolol inhibits angiogenesis, lowers VEGF production, and compromises metastatic potential. In preclinical and clinical studies, combination therapies involving propranolol and chemotherapy, or targeted agents have shown improved efficacy and increased survival, particularly in gastric and breast cancers. Propranolol’s benefits, however, seem to differ depending on the type of cancer, dosage, and length of treatment, and some large cohort studies have not discovered any appreciable reductions in either overall or cancer-specific mortality. These results emphasize the need for additional research to determine the best way to use propranolol in oncology.80 In rare and difficult-to-treat cancers, where conventional drug development is frequently impeded by small patient populations and poor prognoses, the impact of drug repurposing is particularly noteworthy. Repurposing well-known medications lowers expenses, speeds up access to novel treatments, and capitalizes on proven safety profiles—all of which are especially advantageous in environments with limited resources. Experimental screens have found synthetic lethal interactions in aggressive subtypes like PP2A-deficient uterine serous carcinoma, and computational analyses using large-scale cancer genomics datasets have shown that most rare cancer samples contain potential repurposing opportunities. Patients with rare cancers treated with repurposed agents, such as ribonucleotide reductase inhibitors in uterine serous carcinoma and the photosensitizer TLD1433 in conjunctival melanoma, appear to have better results, according to retrospective clinical data. Web-based tools and data-driven methodologies support these efforts by making it easier to identify repurposing candidates based on drug-target interactions, chemical structure, and disease-gene associations.81
Utilizing benefits like shortened time and cost to market, pre-existing supply chains, and the possibility of combination therapies, drug repurposing also provides a universal approach for neglected and challenging-to-treat cancers. Drugs with genetically supported targets have a higher chance of succeeding in clinical development, and advances in genomics and network biology have made it possible to identify repurposing candidates by connecting disease-associated genes with drug targets. Drug repurposing is still a viable and effective strategy for increasing therapeutic options in oncology, despite obstacles relating to data quality, patient heterogeneity, cost, intellectual property, and regulatory requirements. The use of antifungal medications like clotrimazole and ketoconazole for their anticancer effects and the combination of metformin and thymoquinone to treat leukemia’s drug resistance are noteworthy examples. The ability of repurposed medications to address resistance mechanisms that restrict the effectiveness of conventional therapies is demonstrated by the antifungal itraconazole’s ability to reverse docetaxel resistance in prostate cancer.82
In the end, drug repurposing in oncology has produced a number of noteworthy success stories and has a lot of potential going forward, especially for uncommon and challenging-to-treat cancers. The combination of experimental, computational, and molecular methods has increased the range of treatments that are now available, providing hope for better results in a variety of patient groups. Continued refinement of repurposing strategies, coupled with collaborative efforts across academia, industry, and regulatory agencies, will be essential to realize the full potential of this approach and translate scientific advances into tangible clinical benefits.
Table 2: Key Repurposed Oncology Drugs, Their Mechanisms, and Evidence Level
| Drug | Original Indication | Repurposed Oncology Use | Proposed Mechanism(s) in Cancer | Evidence Level* |
| Metformin | Type 2 Diabetes | Breast, colorectal, prostate, ovarian, head & neck cancers | AMPK activation; mTOR inhibition; reduction in insulin/IGF-1 signaling; anti-proliferative and anti-metastatic effects | Moderate to Strong (multiple Phase II; mixed Phase III) |
| Thalidomide | Sedative (withdrawn) | Multiple myeloma, prostate cancer, cachexia | Anti-angiogenic effects; TNF-α suppression; immunomodulation; molecular glue degrader | Strong (FDA-approved for MM) |
| Propranolol | Hypertension, arrhythmias, anxiety | Angiosarcoma, breast cancer, neuroblastoma, HCC, gastric cancer | β-blockade; anti-angiogenesis; reduced VEGF; apoptosis induction; EMT inhibition | Moderate (preclinical + Phase II signals) |
| Aspirin | Analgesic, anti-inflammatory | Colorectal cancer prevention; adjuvant therapy | COX-2 inhibition; reduced PGE2; antiplatelet effects reducing metastasis | Strong for prevention, Moderate for adjuvant |
| Disulfiram | Alcohol dependence | Breast, lung, prostate cancers | ALDH inhibition; copper-dependent proteasome inhibition; cell death in resistant tumors | Moderate (Phase II trials ongoing) |
| Itraconazole | Antifungal | Lung cancer, prostate cancer, basal cell carcinoma | Hedgehog pathway inhibition; anti-angiogenesis; reversal of drug resistance | Moderate |
| Doxycycline | Antibiotic (tetracycline) | Breast cancer stem cell targeting, melanoma | Mitochondrial inhibition; suppression of CSC metabolism; anti-inflammatory effects | Early-Moderate |
| NSAIDs (e.g., Celecoxib) | Pain, inflammation | Colorectal, breast, lung cancers | COX-2 blockade; apoptosis induction; angiogenesis suppression | Moderate |
| Statins (e.g., Atorvastatin) | Hyperlipidemia | Breast, prostate, hepatocellular cancers | HMG-CoA reductase inhibition; impaired prenylation of oncogenic proteins | Moderate (preclinical + epidemiology) |
| All-trans Retinoic Acid (ATRA) | Dermatologic uses | Acute Promyelocytic Leukemia, NPM1-mutated AML | Differentiation induction; transcriptional reprogramming | Strong (FDA-approved for APL) |
| Chloroquine / Hydroxychloroquine | Antimalarial | Glioblastoma, pancreatic cancer | Autophagy inhibition; lysosomal disruption; sensitization to chemo/radiation | Moderate (ongoing Phase I/II) |
| Famotidine / Cimetidine | GERD & ulcers | Colorectal, gastric cancers | Histamine H2 receptor blockade; immune modulation; anti-adhesion | Early-Moderate |
Implementing Drug Repurposing in Oncology: Obstacles and Restrictions
The regulatory, intellectual property, clinical, biological, and pharmacological aspects of drug repurposing in oncology interact in a complex way to determine the viability and success of converting non-oncology medications into potent cancer treatments. Regulatory considerations are one of the biggest obstacles because before approving new indications for already-approved medications, organizations like the FDA and EMEA need strong proof of efficacy, usually from monotherapy clinical trials. In oncology, where the therapeutic benefit of repurposed agents may only become evident in combination regimens and where the mechanistic justification for synergy is frequently compelling but challenging to prove in isolation, this requirement can be especially onerous. Incentives for formal clinical development may be undermined by the regulatory environment’s requirement for high-quality clinical data, which can be difficult to produce for medications that are already widely accessible and used off-label.83
Issues with intellectual property (IP) make the repurposing process even more difficult. The conventional IP protections that encourage investment in clinical trials and regulatory approval for new indications are frequently absent from repurposed agents, particularly those that are generic or off-patent, in contrast to novel drugs. When there are few chances for market exclusivity and when generic substitution or off-label prescribing can reduce the commercial return on investment, pharmaceutical companies might be hesitant to invest in repurposing initiatives. The time and cost benefits usually associated with repurposing are further diminished when new formulations or dosing regimens are required to maximize efficacy in oncology. This can lead to additional regulatory requirements, such as new phase I trials. Legal ambiguities brought about by the complexity of patent rights, such as those pertaining to novelty and public disclosure, may also discourage industry and academic stakeholders from exploring repurposing opportunities.84 Another significant obstacle in the repurposing paradigm is the design of clinical trials. Phase II trials can be entered more quickly due to the established safety profiles of repurposed medications; however, the success of these trials depends on careful consideration of scheduling, dosing, and patient selection, which may differ significantly from the drug’s original indication. Suboptimal trial designs and inconclusive results have resulted from the failure of many early repurposing trials to take into account mechanistic insights obtained from preclinical studies. Clinical trials should be guided by strong preclinical data, use biomarker-driven patient selection, and modify dosage schedules to attain the best antitumor activity while reducing toxicity in order to increase the chances of success. In order to navigate the changing landscape of evidence standards for repurposed drugs and to align trial design with approval requirements, early and continuous engagement with regulatory authorities is crucial. Additional challenges arise when recruiting patients, especially for rare cancers or trials that need biomarker stratification. Trial accrual may be slowed by the heterogeneity of cancer populations and the requirement for accurate molecular characterization, which may restrict the pool of eligible participants. Off-label use outside of clinical trials may result from the broad availability of repurposed medications for other indications, which could complicate recruitment and possibly skew trial results. Innovative trial designs, like basket or umbrella trials, and adaptable protocols that enable real-time modification based on new data are being used more and more to address these issues.10 One important element of responsible clinical research that improves trial relevance and feasibility is the public’s and patients’ participation in research planning and execution .
One of the main obstacles to the success of drug repurposing in oncology is biological barriers. For instance, the majority of systemically administered medications, including many repurposed agents, are unable to reach therapeutic concentrations in the central nervous system, making the blood-brain barrier (BBB) a significant barrier to treating primary and metastatic brain tumors. To improve drug exposure at the tumor site while reducing systemic toxicity, strategies to improve BBB penetration are being investigated, such as the creation of innovative delivery systems or the application of focused ultrasound. The development of targeted delivery systems, such as nanoparticles or antibody-drug conjugates, is necessary for other cancer types because the tumor microenvironment, which includes elements like hypoxia, stromal barriers, and immune suppression, can restrict drug delivery and efficacy. Using developments in preclinical modeling and drug formulation, efforts are also being made to reevaluate medications that previously failed in clinical trials because of delivery issues.86 Drug resistance, toxicity, and adverse pharmacokinetics are examples of pharmacological barriers, which are intimately related to biological barriers. Drug resistance, whether acquired or intrinsic, is still a major cause of treatment failure in oncology and can reduce the effectiveness of repurposed agents, especially when used as monotherapies. Even FDA-approved medications with favorable pharmacokinetic profiles cannot pass through the blood-spinal cord barrier (BSCB) and blood-brain barrier (BBB) in the context of brain tumors, so alternative delivery methods must be developed.87 Liposomal or nanoparticle formulations are used to increase bioavailability for medications like amino-bisphosphonates because of their quick renal clearance and bone sequestration, which limit systemic exposure and antitumor efficacy.79 Innovative pharmacological solutions are necessary because some cancers, like glioblastoma multiforme, have distinct anatomical and microenvironmental characteristics that make drug delivery even more difficult and increase resistance.
By connecting disease-associated genes with potential drug targets, advances in genomics, network biology, and chemoproteomics continue to propel the search for repurposing candidates in spite of these significant obstacles. Clinical development is more likely to be successful for drugs with genetically supported mechanisms, and the combination of computational and experimental methods is increasing the range of treatments that are currently available. However, it will take consistent work to address regulatory, intellectual property, clinical, biological, and pharmacological challenges through cooperative, multidisciplinary strategies if these discoveries are to be translated into clinical benefit. The development of novel trial designs and delivery systems, the ongoing improvement of these strategies, and the balancing of commercial and regulatory incentives will be necessary for the future of drug repurposing in oncology in order to guarantee that promising treatments reach the patients who need them the most.
Table 3: Regulatory and Commercial Barriers to Drug Repurposing in Oncology
| Barrier Category | Specific Barrier | Description / Impact |
| Regulatory Barriers | Requirement for monotherapy clinical trial evidence | Regulatory agencies (FDA, EMA) often require strong monotherapy data, even when repurposed drugs work best in combination regimens, complicating approval. |
| High standard of proof for new indications | Despite existing safety data, regulators require robust Phase II/III trials, which are costly and time-consuming. | |
| Need for new clinical trials even for known drugs | Modified formulations, new dosing schedules, or combination therapy requires additional regulatory submissions and sometimes new Phase I trials. | |
| Slow approval pathways | Current frameworks were designed for new drugs, making the process inefficient for repurposed agents without dedicated pathways. | |
| Commercial / IP Barriers | Lack of intellectual property protection | Most repurposed drugs are generic/off-patent, reducing commercial incentive to invest in costly clinical trials. |
| Limited market exclusivity | Even if new indications are approved, generic substitution undermines profits, discouraging pharmaceutical industry participation. | |
| Weak financial incentives | Little ability to recoup investment; companies avoid repurposing unless new formulations or new delivery mechanisms can be patented. | |
| Patent challenges & legal ambiguity | Novel use patents are weak, hard to enforce, and often invalidated due to prior public knowledge or off-label use. | |
| Clinical & Operational Barriers | Poor trial enrollment | Patients may choose off-label use instead of clinical trial participation, making recruitment difficult. |
| Heterogeneity of cancer populations | Requires biomarker-based selection; smaller eligible populations increase cost and trial complexity. | |
| Limited access to abandoned or shelved compounds | Lack of centralized repositories limits repurposing of discontinued drugs that could still be effective. | |
| Economic & Policy Barriers | Lack of government incentives | Few policies support repurposing; funding is mainly academic or philanthropic. |
| High cost of evidence generation | Even for known drugs, conducting high-quality clinical trials is expensive, limiting academic-led repurposing. | |
| Misaligned reimbursement systems | Insurance systems may not reimburse repurposed drugs without formal approval, reducing clinical uptake. |
Resources and Cooperation to Support Drug Repurposing Projects
Drug repurposing in oncology has changed as a result of the combined efforts of public-private partnerships, cooperative consortia, and the inclusion of various stakeholders, each of whom has contributed special resources and knowledge to help the field get past its many obstacles. In oncology, where there are significant financial and regulatory barriers, public-private partnerships have become essential to the advancement of drug repurposing. One well-known example is the partnership between the non-profit group Cures Within Reach and the for-profit company Notable Labs. Notable Labs gave Cures Within Reach the commercial rights for pediatric leukemia as part of this collaboration, which resulted in the creation of ND-1000, a repurposed treatment for blood cancers in children and adults. With the help of philanthropic funding and leveraging incentives like the FDA’s Pediatric Priority Review Voucher Program, this arrangement serves as an example of how common interests and resources can lower costs for vulnerable patient populations while facilitating access to innovative therapies. Highlighting the importance of academic participation in translational research, the University of Kansas Cancer Center further enhanced this partnership by contributing clinical trial expertise.88 Additionally, collaborative research consortia have been essential in promoting drug repurposing innovation. For example, the Stowers Institute for Medical Research, Children’s Mercy, and The University of Kansas Cancer Center collaborated to successfully repurpose doxorubicin in order to overcome leukemia resistance. By means of high-throughput screening and validation in animal models and patient-derived samples, the consortium showed that low-dose doxorubicin could improve anticancer immunity and inhibit important molecular pathways, providing a new treatment option for refractory leukemia. These partnerships emphasize how crucial it is to combine clinical knowledge and mechanistic insights in order to maximize the use of current medications in novel oncologic settings. Large-scale consortia like PCM4EU and PRIME-ROSE, which bring together partners from all over Europe to create networks of clinical trials akin to the Drug Rediscovery Protocol (DRUP), have been funded by the European Union at the continental level. By standardizing molecular diagnostics, treatment plans, and reimbursement policies, these programs seek to expedite the adoption of precision cancer medicine an hasten the clinical application of repurposed therapies. The availability and integration of extensive databases and repositories that support drug repurposing research are essential to the success of these collaborative models. For instance, a literature-based resource cataloguing non-cancer medications with evidence of anticancer activity, was created by the Repurposing Drugs in Oncology (ReDO) project. It facilitates systematic literature mining as well as hypothesis generation; Additional noteworthy resources are the Drug Repurposing Hub and the PRISM drug repurposing resource, which together offer curated data on thousands of compounds, their activities, and clinical indications. These resources serve as fundamental tools for computational and experimental repurposing initiatives.89 Additional examples of the expanding ecosystem of informatics tools intended to methodically identify and rank repurposing candidates in oncology include the Predictive Database for Drug Repurposing (PAD) and CADDIE, a web application that integrates gene-gene and drug-gene interaction data; Additional platforms are provided by DrugCentral and DrugRepoBank for ranking applicants according to market exclusivity and intellectual property factors, which are crucial for negotiating the commercial environment of repurposed medications.90
It is still difficult to integrate structured data from preclinical, clinical, and chemical sources because there may not be enough database overlap to allow for thorough analysis. Machine learning and natural language processing to combine data from various sources, such as electronic health records, clinicaltrials.gov, and PubMed, improving the identification of promising repurposing opportunities. The potential for customized repurposing strategies is further increased by the use of biobanks that connect genomic data to clinical outcomes91. Additional resources like RepoDB, CURE ID, the Traditional Chinese Medicine Drug Repurposing Hub, and Broad Drug Repurposing Hub offer open-access platforms for discussing real-world clinical experiences with repurposed therapies, annotating compound activities, and investigating mechanisms of action.92 The scope of resources available to support hypothesis generation and data-driven repurposing is further demonstrated by the Dragon Exploration System for Sickle Cell Disease (DESSCD) and the Cancer-based Pharmacogenomics Network (CPN).93 The development of drug repurposing in oncology is largely dependent on the contributions of stakeholders in academia, government, and business. The majority of the evidence in favor of using off-patent medications for cancer has traditionally come from academia and independent researchers, frequently concentrating on generic medications with well-established safety profiles. However, academic groups may find it more difficult to obtain marketing exclusivity and handle the intricate approval process if they lack regulatory knowledge and intellectual property protections. As a result, collaborations with businesses and nonprofits have grown more alluring since they bring together academic creativity with the business and legal knowledge required for successful translation.94
Oncology drug repurposing’s future hinges on these cooperative models’ ongoing development, the incorporation of extensive data sources, and the balancing of business and regulatory incentives. To fully realize the potential of repurposed therapies, more funding for academically driven research, improved regulatory support, and the creation of creative trial designs are necessary. The combined efforts of academia, industry, government, and non-profit organizations will be essential in enhancing the therapeutic arsenal and improving outcomes for cancer patients as the disease’s incidence and financial burden continue to rise globally.95- 99
Conclusion
Drug repurposing has become a promising strategy in oncology, offering faster, safer, and more cost-effective therapeutic development by leveraging existing drugs with established safety profiles. Advances in computational biology, multi-omics technologies, and AI-driven prediction platforms have significantly improved the identification of repurposing candidates with strong mechanistic relevance. These approaches have already produced a number of clinical successes, particularly in rare and treatment-resistant cancers.
Despite these achievements, major barriers persist, including regulatory constraints, limited intellectual property protection, and inconsistent clinical validation across diverse patient populations. Tumor heterogeneity, lack of robust biomarkers, and challenges in translating preclinical findings into durable clinical responses further complicate progress.
To fully realize the potential of drug repurposing, stronger collaborative frameworks, improved patient stratification, and more rigorous prospective trials are urgently needed. Enhancing data integration, supporting academic-industry partnerships, and creating regulatory and economic incentives will accelerate the translation of repurposed agents into routine oncology practice. Ultimately, a coordinated, multidisciplinary effort will be essential for delivering more accessible and effective cancer therapies through repurposing.
Acknowledgement
I extend my sincere gratitude to the researchers, clinicians, and scientific communities whose significant contributions have enriched the field of drug repurposing in oncology and supported the development of this manuscript. I am deeply thankful to the authors of the referenced studies whose rigorous work has laid the scientific foundation for this review. My appreciation also goes to the institutions and collaborative networks that continue to promote interdisciplinary efforts in pharmacology, oncology, computational science, and regulatory research. Finally, this work is dedicated to the global oncology community and to the patients and families whose resilience continues to inspire progress in advancing repurposed therapeutics for improved cancer care.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The author(s) declare that there is no conflict of interest regarding the publication of this review.
Conflict of interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from other sources
Not Applicable
Author Contributions
Evangeline Joan Arockiadoss: contributed to the conceptualization of the review, drafting of the sections on Introduction, What Is Drug Repurposing in the Oncology Context?, and Methods and Strategies for Drug Repurposing in the Treatment of Cancer. She also participated in the literature search, organization of content, and preparation of the initial manuscript draft.
Shibin Ramchandran: contributed to the development of the article structure, writing of the sections on Oncology Drug Repurposing Success Stories, Implementing Drug Repurposing in Oncology: Obstacles and Restrictions, and Resources and Cooperation to Support Drug Repurposing Projects. He also guided the critical revision of the manuscript, supervised the scientific accuracy, and designed the graphical abstract. Both authors contributed to the Conclusion, review and editing of the full manuscript, and approved the final version of the article.
Reference
- Pushpakom S, Iorio F, Eyers PA, et al. Drug repurposing: Progress, challenges and recommendations. Nat Rev Drug Discov. 2019;18(1):41-58. doi:10.1038/nrd.2018.168.
CrossRef - Zhang M, Zhang L, Zou J, Yao C. Drug repurposing for cancer therapy. Signal Transduct Target Ther. 2024;9:191. doi: 10.1038/s41392-024-01808.
CrossRef - Pantziarka P, Bouche G, Meheus L, Sukhatme V, Sukhatme VP. The Repurposing Drugs in Oncology (ReDO) Project. ecancer. 2014;8:442. doi: 10.3332/ecancer.2014.485.
CrossRef - Lord-Bessen J.J, Stewart D.J, Haaland B.C. Drug repurposing in oncology—patient and health systems opportunities. Nat Rev Clin Oncol. 2015;12:59-71. doi: 10.1038/nrclinonc.2015.169.
CrossRef - Müller S, Kraus S. Drug repurposing of generic drugs: Challenges and the potential role for government. Appl Health Econ Health Policy. 2023;21(3):345-358. doi: 10.1007/s40258-023-00816-6.
CrossRef - Hirt, C. K., Booij, T. H., Grob, L., Simmler, P., Toussaint, N. C., Keller, D., … & Schwank, G. Drug screening and genome editing in human pancreatic cancer organoids identifies drug–gene interactions and candidates for off-label treatment. Cell Genomics. 2022;2:100120. doi: 10.1016/j.xgen.2022.100095.
CrossRef - Vivarelli S, Candido S, Caruso G, Falzone L, Libra M. Patient-derived tumor organoids for drug repositioning in cancer care. Cancers. 2020;12:. doi: 10.3390/cancers12123636.
CrossRef - Walpole, I. R., Zaman, F. Y., Zhao, P., Marshall, V. M., Lin, F. P., Thomas, D. M., & Ameratunga, M. Computational repurposing of oncology drugs through off-target drug binding interactions. Clin Transl Med. 2024;14:. doi: 10.1002/ctm2.1657.
CrossRef - Shah R.R, Stonier P.D. Repurposing old drugs in oncology: Opportunities with clinical and regulatory challenges ahead. J Clin Pharm Ther. 2019;44:. doi: 10.1111/jcpt.12759.
CrossRef - Lee, W. H., Loo, C. Y., Ghadiri, M., Leong, C. R., Young, P. M., & Traini, D. The potential to treat lung cancer via inhalation of repurposed drugs. Adv Drug Deliv Rev. 2018;133:107-125. doi: 10.1016/j.addr.2018.08.012.
CrossRef - Siddiqui S, Deshmukh A.J, Mudaliar P, Nalawade A.J, Iyer D, Aich J. Drug repurposing: Re-inventing therapies for cancer. J Egypt Natl Cancer Inst. 2022;34:33. doi: 10.1186/s43046-022-00137-0.
CrossRef - DeVita V.T, Chu E. A history of cancer chemotherapy. Cancer Res. 2008;68(21):8643-8653. doi: 10.1158/0008-5472.CAN-07-6611.
CrossRef - Quirke V.M. Tamoxifen from failed contraceptive pill to best-selling breast cancer medicine. Front Pharmacol. 2017;8:620. doi: 10.3389/fphar.2017.00620.
CrossRef - Pushpakom, S., Iorio, F., Eyers, P. A., Escott, K. J., Hopper, S., Wells, A., … & Pirmohamed, M. Drug repurposing: Progress, challenges and recommendations. Nat Rev Drug Discov. 2019;18(1):41-58. doi: 10.1038/nrd.2018.168.
CrossRef - Pantziarka P, Bouche G, Meheus L, Sukhatme V, Sukhatme VP. Repurposing drugs in oncology—cimetidine as an anti-cancer agent. ecancermedicalscience. 2014;8:485. doi: 10.3332/ecancer.2014.485.
CrossRef - Krishnamurthy N, Grimshaw AA, Axson SA, Choe SH, Miller JE. Drug repurposing: A systematic review on root causes, barriers and facilitators. BMC Health Serv Res. 2022;22:970. doi: 10.1186/s12913-022-08272-z.
CrossRef - Inoue Y, Song T, Wang X, Luna A, Fu T. DrugAgent: Multi-agent LLM-based reasoning for drug–target interaction prediction. 2025;2408. doi: 10.48550. 2408.13378.
- Menden, M. P., Iorio, F., Garnett, M., McDermott, U., Benes, C. H., Ballester, P. J., & Saez-Rodriguez, J. Machine learning prediction of cancer cell sensitivity to drugs. PLoS One. 2013;8(4):e61318. doi: 10.1371/journal.pone.0061318.
CrossRef - Baranda J.C, Godwin A.K. Advancing the promises of precision medicine for GIST. Gastrointest Stromal Tumor. 2019;2:. doi: 10.21037/gist.2019.10.01.
CrossRef - Reichardt P. The story of imatinib in GIST: a journey through the development of targeted therapy. Oncol Res Treat. 2018;41(7-8):472-477. doi: 10.1159/000487511.
CrossRef - Calderwood S.K. Tumor heterogeneity, clonal evolution, and therapy resistance. Discov Med. 2013;15(82):188-195. doi: 10.1016/S1531-8416(13)70033-6.
- West J, You L, Zhang J, Gatenby R.A, Brown J.S, Newton P.K, Anderson A.R. Towards multidrug adaptive therapy. Cancer Res. 2020;80(7):1578-1589. doi: 10.1158/0008-5472.CAN-19-2669.
CrossRef - Catenacci D.V. Next-generation clinical trials: addressing tumor molecular heterogeneity. Mol Oncol. 2015;9(5):967-976. doi: 10.1016/j.molonc.2014.09.011.
CrossRef - Tian Y, Wang X, Wu C, Qiao J, Jin H, Li H. A protracted war against cancer drug resistance. Cancer Cell Int. 2024;24:326. doi: 10.1186/s12935-024-03510-2.
CrossRef - Ma C, Zhou Z, Liu H, Koslicki D. KGML-xDTD: a knowledge graph–based machine learning framework for drug treatment prediction. GigaScience. 2023;12:057. doi: 10.1093/gigascience/giad057.
CrossRef - Inoue Y, Song T, Wang X, Luna A, Fu T. DrugAgent: Multi-agent LLM reasoning for drug–target prediction. 2025; 2408. doi: 10.1002/wcms.1597.
CrossRef - Pan X, Lin X, Cao D, Zeng X, Yu PS, He L, Nussinov R, Cheng F. Deep learning for drug repurposing. Wiley Interdiscip Rev Comput Mol Sci. 2022;12:1597. doi: 10.1002/wcms.1597.
CrossRef - Yang C, Zhang H, Chen M, Wang S, Qian R, Zhang L, et al. Signature-based drug repositioning for liver cancer. eLife. 2022;11:71880. doi: 10.7554/eLife.71880.
CrossRef - Cheng J, Yang L, Kumar V, Agarwal P. Evaluation of connectivity map. Genome Med. 2014;6(12):95. doi: 10.1186/s13073-014-0095-1
CrossRef - McCabe B, Liberante F, Mills KI. Repurposing medicinal compounds for blood cancer. Ann Hematol. 2015;94(8):1267-1276. doi: 10.1007/s00277-015-2412-1
CrossRef - Carlos-Escalante, J. A., Gomez-Flores-Ramos, L., Bian, X., Perdomo-Pantoja, A., de Andrade, K. C., Mejía-Pérez, S. I., … & Wegman-Ostrosky, T. Germline variants in AGT, MGMT, TP53 in Mexican astrocytoma patients. Cell Mol Neurobiol. 2021;41(6):1285-1297. doi: 10.1007/s10571-020-00901-7.
CrossRef - Paul SM, Mytelka DS, Dunwiddie CT, Persinger CC, Munos BH, Lindborg SR, Schacht AL. How to improve R&D productivity: the pharmaceutical industry’s grand challenge. Nat Rev Drug Discov. 2010;9(3):203-214. doi:10.1038/nrd3078.
CrossRef - Roder C, Thomson M.J. Auranofin: repurposing an old drug. Drugs R D. 2015;15(1):13-20. doi: 10.1007/s40268-015-0083-y.
CrossRef - Banerjee J, Tiwari A.K, Banerjee S. Drug repurposing for cancer. Prog Mol Biol Transl Sci. 2024;207:123-150. doi: 10.1016/bs.pmbts.2024.03.032.
CrossRef - Banerjee S, Banerjee J, Tiwari AK. Functional genomics and human diseases. In: Advances in Genomics. 2024:141-166. doi: 10.1007/978-981-97-3169-5_7.
CrossRef - Abdelaleem, M., Ezzat, H., Osama, M., Megahed, A., Alaa, W., Gaber, A., & Refaat, A. Prospects for repurposing CNS drugs for cancer. Oncol Rev. 2019;13(1):411. doi: 10.4081/oncol.2019.411.
CrossRef - Hsu, C. C., Peng, D., Cai, Z., & Lin, H. K. Drug repurposing as strategy for cancer therapy. Semin Cancer Biol. 2021;68:258-278. doi: 10.1016/j.semcancer.2021.04.006.
CrossRef - Gonzalez-Fierro A, Duenas-Gonzalez A. Drug repurposing for cancer therapy. Semin Cancer Biol. 2021;68:123-131. doi: 10.1016/j.semcancer.2019.12.012.
CrossRef - Verbaanderd C, et al. ReDO: chloroquine and hydroxychloroquine as anticancer agents. ecancermedicalscience. 2017;11:781. doi: 10.3332/ecancer.2017.781.
CrossRef - Xia Y, Sun M, Huang H, Jin W. Drug repurposing for cancer therapy. Signal Transduct Target Ther. 2024;9:92. doi: 10.1038/s41392-024-01808-1.
CrossRef - Malla, R., Viswanathan, S., Makena, S., Kapoor, S., Verma, D., Raju, A. A., … & Muniraj, N. Revitalizing cancer treatment through drug repurposing. Cancers. 2024;16. doi: 10.3390/cancers16081463.
CrossRef - Islam S, Wang S, Bowden N, Martin J, Head R. Kinase-targeted repurposing in oncology. Br J Clin Pharmacol. 2022;88. doi: 10.1111/bcp.14964.
CrossRef - Regulska, K., Regulski, M., Karolak, B., Murias, M., & Stanisz, B. Can cardiovascular drugs support cancer therapy? Drug Discov Today. 2019;24. doi: 10.1016/j.drudis.2019.03.010.
CrossRef - Xu X, Sun M, Huang H, Jin W. Molecular network–based drug prediction in thyroid cancer. Int J Mol Sci. 2019;20:396. doi: 10.3390/ijms20020396.
CrossRef - Tripathi S, Gupta E, Galande S. Statins as anti-tumor agents. Cancer Rep. 2024;7:1820. doi: 10.1002/cnr2.2078.
CrossRef - Kim Y, Lee H. CRISPR-Cas for identifying drug combinations. Cells. 2023;12. doi: 10.3390/cells12222593.
CrossRef - Weth FR, Hoggarth G, et al. Advances in repurposing drugs for cancer therapy. Br J Cancer. 2024;130(5):703-715. doi: 10.1038/s41416-023-02502-9.
CrossRef - Giuliano, A., Horta, R. S., Vieira, R. A., Hume, K. R., & Dobson, J. Repurposing drugs in small animal oncology. Animals. 2022;12. doi: 10.3390/ani13010139.
CrossRef - Xia Y, Sun M, Huang H, Jin W. Drug repurposing for cancer therapy. Signal Transduct Target Ther. 2024;9:92. doi: 10.1038/s41392-024-01808-1.
CrossRef - Wan Z, Sun X, Li Y, Chu T, Hao X, Cao Y, Zhang P. Applications of artificial intelligence in drug repurposing. Adv Sci. 2025;12(14):2411325. doi: 10.1002/advs.202411325.
CrossRef - Sajwani N, Suchitha G.P, Keshava Prasad TS, Dagamajalu S. Drug repurposing in oncology: A path beyond the bottleneck. Med Oncol. 2025;42(10):443. doi: 10.1007/s12032-025-02994-w.
CrossRef - van der Pol K.H, Aljofan M, Blin O, Cornel J.H, Rongen G.A, Woestelandt A.G, Spedding M. Drug repurposing of generic drugs: challenges and the government role. Appl Health Econ Health Policy. 2023;21(6):831-840. doi: 10.1007/s40258-023-00816-6.
CrossRef - Hernandez JJ, Pryszlak M, Smith L, Yanchus C, Kurji N, Shahani VM, Molinski SV. Overcoming regulatory hurdles in repurposing drugs as cancer therapeutics. Front Oncol. 2017;7:273. doi: 10.3389/fonc.2017.00273.
CrossRef - Ghislat G, Hernandez-Hernandez S, Piyawajanusorn C, Ballester PJ. Data-centric challenges in AI for drug discovery. Expert Opin Drug Discov. 2024;19(11):1297-1307. doi: 10.1080/17460441.2024.2403639.
CrossRef - Bhar S. Role of drug repurposing in sustainable drug discovery. In: Drug Repurposing–Advances and Opportunities. 2023:23-45. doi: 10.5772/intechopen.110621.
CrossRef - Corsello S.M, Nagari R.T, Spangler R.D, Rossen J, Kocak M, Bryan J.G, et al. Discovering anticancer potential of non-oncology drugs. Nat Cancer. 2020;1(2):235-248. doi: 10.1038/s43018-019-0018-6.
CrossRef - Massart D, Zeicher M. Qibitz: Mining PubMed for repurposable drugs. 2024;2412.12363. doi: 10.48550/2412.12363.
- Talamo G, Dolloff N.G, Sharma K, Zhu J, Malysz J. Plasma cell leukemia: clinical features and outcomes. Rare Tumors. 2012;4:. doi: 10.4081/rt.2012.e39.
CrossRef - Prado B.L, Qian Y. Anti-cytokines in treatment of cancer cachexia. Ann Palliat Med. 2019;8:. doi: 10.21037/apm.2018.07.06.
CrossRef - Landgren O, Iskander K. Modern multiple myeloma therapy. J Intern Med. 2017;281:365-382. doi: 10.1111/joim.12590.
CrossRef - Liu, Y., He, S., Ding, Y., Huang, J., Zhang, Y., & Chen, L. Thalidomide-based therapy in NSCLC: meta-analysis. Contemp Oncol. 2014;18:36-44. doi: 10.5114/wo.2014.40782.
CrossRef - Pandey S, Bradley L, Del Fabbro E. Updates in cancer cachexia. Cancers. 2024;16:. doi: 10.3390/cancers16091696.
CrossRef - Li-J.M, Jun Wang, Wei-F.F, Xiao-L.P, Fu-YL, Min Y. Evaluation of oral chemotherapy with capecitabine and cyclophosphamide plus thalidomide and prednisone in prostate cancer patients. J Cancer Res Clin Oncol. 2012 Feb;138(2):333–339. DOI: 10.1007/s00432-011-1101-2.
CrossRef - Frere G.A, de Araujo E.D, Gunning P.T. Targeted protein degradation by molecular glues. Methods Cell Biol. 2022;185:1-33. doi: 10.1016/bs.mcb.2022.01.001.
CrossRef - Heckman-Stoddard B.M, DeCensi A, Sahasrabuddhe V.V, Ford L.G. Repurposing metformin for cancer prevention. Diabetologia. 2017;60:1639-1647. doi: 10.1007/s00125-017-4372-6.
CrossRef - Franciosi, M., Lucisano, G., Lapice, E., Strippoli, G. F., Pellegrini, F., & Nicolucci, A. Metformin therapy and cancer risk. PLoS One. 2013;8:66537. doi: 10.1371/journal.pone.0071583.
CrossRef - Gaertner F, Preissner S, Heiland M, Preissner R, Wüster J. Metformin and five-year survival in head and neck cancer. Cancers. 2024;16:. doi: 10.3390/cancers16050982.
CrossRef - Belda-Iniesta C, Pernía O, Simó R. Metformin: a new option in cancer treatment. Clin Transl Oncol. 2011;13:363-367. doi: 10.1007/s12094-011-0669-y.
CrossRef - Pácal L, Kaňková K. Metformin in oncology repurposing status. Klin Onkol. 2020;33:87-94. doi: 10.14735/amko2020107.
CrossRef - Christodoulou M.I, Scorilas A. Metformin in anti-cancer therapies. Curr Med Chem. 2017;24:1-13. doi: 10.2174/0929867324666170203095715.
CrossRef
- Coyle C, Cafferty F.H, Vale C, Langley R.E. Metformin as adjuvant therapy for cancer. Ann Oncol. 2016;27:2184-2195. doi: 10.1093/annonc/mdw410.
CrossRef - Kheirandish M, Mahboobi H, Yazdanparast M, Warda K, Kamal M.A. Anti-cancer effects of metformin. Curr Drug Metab. 2018;19:. doi: 10.2174/1389200219666180416161846.
CrossRef - Ahmed, Z. S., Golovoy, M., Abdullah, Y., Ahmed, R. S. I., & Dou, Q. P. Repurposing metformin for cancer: patent review. Recent Pat Anticancer Drug Discov. 2021;16:. doi: 10.2174/1574892816666210615163417.
CrossRef - Samsuri N.A, Leech M, Marignol L. Metformin in radiation therapy. Cancer Treat Rev. 2017;55:150-162. doi: 10.1016/j.ctrv.2017.03.005.
CrossRef - Bosso M, Haddad D, A.l Madhoun A, Al-Mulla F. Targeting cancer and diabetes metabolic overlap. Biomedicines. 2024;12. doi: 10.3390/biomedicines12010211.
CrossRef
- Galal, M. A., Al-Rimawi, M., Hajeer, A., Dahman, H., Alouch, S., & Aljada, A. Metformin in cancer treatment and prevention. Int J Mol Sci. 2024;25:. doi: 10.3390/ijms25074083.
CrossRef - Zhang HH, Guo XL. Metformin and chemotherapy synergy. Cancer Chemother Pharmacol. 2016;78:109-117. doi: 10.1007/s00280-016-2962-y.
CrossRef - Provinciali, N., Lazzeroni, M., Cazzaniga, M., Gorlero, F., Dunn, B. K., & DeCensi, A. Metformin risk–benefit profile in cancer. Expert Opin Drug Saf. 2015;14:1709-1719. doi: 10.1517/14740338.2015.1084289.
CrossRef - Wolter, J. K., Wolter, N. E., Blanch, A., Partridge, T., Cheng, L., Morgenstern, D. A., … & Irwin, M. S. Propranolol anti-tumor activity in neuroblastoma. Oncotarget. 2014;5. doi: 10.18632/oncotarget.1083.
CrossRef - Cao J, Chow L, Dow S. Overcoming immune suppression in the tumor microenvironment. Front Oncol. 2023;13:. doi: 10.3389/fonc.2023.1116016.
CrossRef - Chang, P. Y., Huang, W. Y., Lin, C. L., Huang, T. C., Wu, Y. Y., Chen, J. H., & Kao, C. H. Propranolol reduces cancer risk. Medicine. 2015;94:1097. doi: 10.1097/MD.0000000000001097.
CrossRef - Gales, L., Forsea, L., Mitrea, D., Stefanica, I., Stanculescu, I., Mitrica, R., … & Serbanescu, L. Co-adjuvant drugs in cancer therapy. Medicina. 2022;58. doi: 10.3390/medicina58091239.
CrossRef - Albiñana, V., Gallardo-Vara, E., Casado-Vela, J., Recio-Poveda, L., Botella, L. M., & Cuesta, A. M. Propranolol in benign tumors and cancer. J Clin Med. 2022;11. doi: 10.3390/jcm11154539.
CrossRef - Mravec B, Horvathova L, Hunakova L. β-adrenergic signaling in cancer. Int J Mol Sci. 2020;21:7988. doi: 10.3390/ijms21217988.
CrossRef - Hu Q,, Propranolol induces apoptosis in gastric cancer. Front Oncol. 2021;11:620101. doi: 10.3389/fonc.2021.620101.
CrossRef - Archer, M., Dogra, N., Dovey, Z., Ganta, T., Jang, H. S., Khusid, J. A.,& Kyprianou, N. Role of α- and β-adrenergic signaling in urologic cancers. Cell Commun Signal. 2021;19:44. doi: 10.1186/s12964-021-00755-6.
- Cardwell, C. R., Pottegård, A., Vaes, E., Garmo, H., Murray, L. J., Brown, C., … & Bennett, K. Propranolol and survival in breast cancer. Breast Cancer Res. 2016;18:119. doi: 10.1186/s13058-016-0782-5.
CrossRef - Barbieri, A., Robinson, N., Palma, G., Maurea, N., Desiderio, V., & Botti, G. β2-adrenergic pathway and inflammation in cancer and COVID-19. Front Immunol. 2020;11:581. doi: 10.3389/fimmu.2020.588724
CrossRef - Lee, P. C., Chen, Y. J., Chou, Y. C., Lee, K. C., Chen, P. H., Kao, W. Y., … & Su, C. W. Low-dose propranolol improves survival in cirrhosis. Eur J Gastroenterol Hepatol. 2020;32:336-343. doi: 10.1097/MEG.0000000000001511
CrossRef - Suna, N., Öcal, S., & Selçuk, H. Propranolol reduces HCC incidence in cirrhosis. Exp Clin Transplant. 2019;17:208-215. doi: 10.6002/ect.2018.0321.
CrossRef - Zhao, S., Fan, S., Shi, Y., Ren, H., Hong, H., Gao, X., … & Li, H. Propranolol induces apoptosis in ovarian cancer. J Cancer. 2020;11:2410-2420. doi: 10.7150/jca.46556.
CrossRef - Peixoto R, Pereira ML, Oliveira M. Beta-blockers and cancer. Pharmaceuticals. 2020;13:. doi: 10.3390/ph13060105.
CrossRef - Boyer, A., Pasquier, E., Tomasini, P., Ciccolini, J., Greillier, L., Andre, N., … & Mascaux, C.. Drug repurposing in mesothelioma. Eur Respir Rev. 2018;27:170116. doi: 10.1183/16000617.0098-2017.
CrossRef - Walpole IR, Zaman FY, Zhao P, Marshall VM, Lin F, Thomas DM, Shackleton M, Antolin A, Ameratunga M. Clin Transl Med. 2024;14: e1657. doi: 10.1002/ctm2.1657
CrossRef - Carcinoma. O’Connor CM, Taylor SE, Miller KM, et al. Cancer Res. 2022;82(4):721-733. doi: 10.1158/0008-5472.CAN-21-1987
CrossRef - Wang, Y., Aldahdooh, J., Hu, Y., Yang, H., Vähä-Koskela, M., Tang, J., & Tanoli, Z. Sci Rep. 2022;12:5555. doi:10.1038/s41598-022-24980-2
CrossRef - Chen, Q., Ramu, V., Aydar, Y., Groenewoud, A., Zhou, X. Q., Jager, M. J., … & Snaar-Jagalska, B. E. Cancers. 2020;12:2914. doi:10.3390/cancers12030587
CrossRef - Lima, T. S., Souza, L. O., Iglesias-Gato, D., Elversang, J., Jørgensen, F. S., Kallunki, T., … & Moreira, J. M. Front Pharmacol. 2022;13:869461. doi: 10.3389/fphar.2022.869461
CrossRef
Abbreviations
AI – Artificial Intelligence
BBB – Blood–Brain Barrier
BSCB – Blood–Spinal Cord Barrier
CNS – Central Nervous System
FDA – Food and Drug Administration
GIST – Gastrointestinal Stromal Tumor
IMiD – Immunomodulatory Drug
IP – Intellectual Property
MM – Multiple Myeloma
NCATS – National Center for Advancing Translational Sciences
NSCLC – Non-Small Cell Lung Cancer
PI3K – Phosphatidylinositol-3-Kinase
TME – Tumor Microenvironment
VEGF – Vascular Endothelial Growth Factor
Accepted on: 15-12-2025
Second Review by: Dr. Nafees Ahamad
Final Approval by: Dr. Wagih Ghannam








![]()
![]()
