

Manuscript accepted on : 01 September 2016
Published online on: --
Plagiarism Check: Yes
Effect of N-Acetyl Cysteine on Liver Function in General Anesthesia with Isoflurane
Bijan Yazdi1, Alireza Jahangiri Fard2, Saber Akhtaran3, Mohammad Khalili4 and Behnam Mahmoodiyeh1*
1Department of Anesthesia and Critical Care , Arak University of Medical Sciences , Arak , Iran.
2Fellowship of Cardiac Anesthesia, Tracheal Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD) ,Shahid Beheshti University of Medical Science, Tehran, Iran.
3Aneshtesiologist , Arak University of Medical Sciences , Arak , Iran.
4Department of anesthesia and critical care ,Anesthesiologist,Arak University of Medical Science , Arak ,Iran.
Corresponding Author E-mail: behnammahmoodiyeh@gmail.com
DOI : http://dx.doi.org/10.13005/bbra/2294

ABSTRACT: The occurrence of toxicity in various organs was examined since volatile anesthetics have been used clinically. Among the complications the liver toxicity is very important. Due to the effects of N-Acetyl Cysteine (NAC), we decided to conduct a study to assess liver function in patients undergoing anesthesia with isoflurane and received NAC to evaluate its effects on the liver complications of these anesthetics. In this double-blind clinical trial, 68 patients between 20 to 60 years old candidate for elective surgery with a time duration between 1 to 3 hours (except surgeries on the liver and biliary tract) were enrolled and randomly divided into two groups, N-acetylcysteine and control. To check liver function, the levels of AST, ALT, LDH, PT, aPTT and INR was measured in the preoperative, 1 hour and 24 hours after surgery. The results of the study showed that there was significant difference between the levels of ALT (p=0.0001), AST (p=0.0001), and LDH (p=0.0001) between two groups. Heart rate was also significantly different between groups (p=0.0001) but the difference in systolic (p=0.096) and diastolic (p=0.174) blood pressure was not significant. N-acetyl cysteine is an antioxidant medication and its effects on excreting organs such as the kidneys and liver is frequently evaluated. In this study, n-acetyl cysteine could significantly reduce liver enzyme levels after administration of isoflurane, compared to the control group.
KEYWORDS: Key Words: Acetylcysteine, Isoflurane, Liver, Toxicity.
Download this article as:| Copy the following to cite this article: Yazdi B, Fard A. J, Akhtaran S, Khalili M, Mahmoodiyeh B. Effect of N-Acetyl Cysteine on Liver Function in General Anesthesia with Isoflurane. Biotech Res Asia 2016;13(3). |
| Copy the following to cite this URL: Yazdi B, Fard A. J, Akhtaran S, Khalili M, Mahmoodiyeh B. Effect of N-Acetyl Cysteine on Liver Function in General Anesthesia with Isoflurane. Biotech Res Asia 2016;13(3). Available from: https://www.biotech-asia.org/?p=15965 |
Introduction
The occurrence of toxicity in various organs was examined since volatile anesthetics have been used clinically (1, 2). Among the complications, the liver toxicity is very important as liver is the organ which is responsible for the metabolism of these medicines. So far, there have been numerous reports about occurrence of hepatitis after operation under halothane anesthesia whose degree ranged from little rise of Bilirubin to liver Fulminant necrosis (3).
Although isoflurane is less hepatotoxic than halothane, recent reports show the occurrence of liver complications with these anesthetic gases (2, 4). These gases are not toxic by themselves, but their metabolism results in products which are toxic (5). Isoflurane is a halogenated ether and an Isomer of enflurane. Induction of anesthesia with it is much faster than halothane as it is insoluble in blood. Only 0.17% of it is metabolized in liver and its metabolites are fluoride and tri-fluoro acetic acid (TFA). TFA is a reactant metabolite and it is considered to be the main cause of hepatotoxicity. This factor is attached to hepatocyte proteins and acts as a Hapten. Then, antibodies are produced against this Hapten (5).
Toxicity with volatile anesthesia usually takes place after their decomposition in the body and this molecular decomposition results in peroxidation of fats. N-acetylcysteine (NAC) is the acetylated compound of L-cysteine amino acid which can also act as the source of sulfhydryl groups. In our body, this material turns into metabolites which stimulate glutathione and result in detoxification and discharge of free radicals. Prescription of NAC as a mucolytics has been used since a long time ago. Seemingly, this medicine can be really effective in the cases when the level of GSH has decreased significantly or in the condition when the body faces a large accumulation of oxidative materials (HIV infections, cancer, cardiovascular disease, etc). NAC seems to have useful effects in absorption of heavy metals in the case of toxicities and protects the liver and kidney from their negative effects and improves their disposal. This medicine is mostly used to treat toxication with acetaminophen and those patients suffering from COPD, inflammatory diseases of the joints, ARDS, etc (6-9).
Keeping in mind the effects of NAC, we decided to conduct a research on the performance of the liver of those patients under anesthesia with isoflurane who receive NAC and study the effects of this medicine on liver complications of these anesthetics.
Materials and Method
In this double-blind clinical trial, 68 ASA patients aging 20 to 60 in class I-II who had applied for elective surgery with a length of 1-3 hours (except for the operations conducted on liver and biliary ducts) who had resorted to Valiasr Hospital of Arak were chosen and randomly divided into 2 groups. The patients would be excluded from the research if they had a record of hepatitis B and C, IBD, cardiovascular, pulmonary, kidney, and liver disease or consumption of warfarin, aspirin, NSAIDS, vitamins, corticosteroids, immunity weakening medicines or any medicine that intervenes the metabolic performance of the liver, smoking cigarettes or any other narcotics, drinking alcohol, malabsorption, infections (with/without fever) and abdominal surgery over the last 5 years.
According to medical ethics principles, the necessary steps were taken to gain the consent of patients to enter the project.
All the patients underwent physical examination on the day preceding the surgery. They received no prodrugs before entering the operation room and their ages, genders and weights were registered. In the operation room, their IV was taken using No. 20 angiocath from behind their hand and infusion of normal saline started. By basic monitoring before induction of anesthesia and during standard ECG operation (5 leads), blood pressure and arterial oxygen saturation were measured. Heart beat, systolic and diastolic blood pressure and average blood pressure and saturated percentage of oxygen () were measured and registered.
In the first group, 150 mg/kg NAC was poured into 250 ml normal saline and isoflurane medicine was used to retain anesthesia. In the second group, only 250 ml normal saline was injected and isoflurane was used to sustain anesthesia.
Before induction of anesthesia, all the patients were pre-oxygenated with 100% oxygen and they were all given Fentanyl prodrug with a dose of 2 mcg/kg, 3-6 mg/kg sodium Thiopental prodrug (logi Chem UK) and 0.5 mg/kg Atracurium (Alborz Darou). Intubation was carried out 3 minutes later. During anesthesia and based upon the group of patient, a mixture of 50% oxygen gas, 50% N2O and 1-2 MAC isoflurane was used. The current volumes was set to 6-8 ml/kg and the number of breaths was set to 10-12 per minute.
Hemodynamic parameters such as HR, SAD, DAP, MAP, SPO2 were measured every 10 minutes before induction of anesthesia, immediately after induction of anesthesia, and after intubation until the operation was over. In the case of any symptoms indicating reduction anesthesia level, pupillary dilatation, autonomic responses such as sweating, shedding tears, somatic responses (such as movement of organs, raising eyebrows, opening the eyes), a 20% rise in blood pressure and heart beat, the amount of anesthetic gas prescribed was increased as much as 1 MAC. When the heart beat and blood pressures decreased more than 20%, the amount of anesthetic gas was reduced again.
During anesthesia, all patients received 1 mg/kg Fentanyl and 0.2 mg/kg Atracurium every 40 minutes. As for those groups which had received NAC during induction of anesthesia, infusion of 12.5 mg/kg of this medicine continued throughout the operation. As for the other groups, only normal saline infusion was carried out.
To study the liver’s performance, the level of INR, aPTT, PT, LDH, ALT, and AST was checked before, 1 hour, and 24 hours after the operation (Iran-made Pars Azmoon kits were used for AST, ALT, LDH enzymes, while German Fischer kits were utilized for PT and aPTT).
In the face of any complications during the surgery such as arrhythmia, Hypotension for more than 15 minutes resistant to treatment, need for injection of blood products, using medicines that influence the liver blood flow such as Beta blocker, vomiting, nausea, flushing, cough, and Urticaria during pre-operation stages, these complications were recorded. If these complications occurred while injecting NAC, the patient would be excluded from research. The person in charge of registering and recording the information had no information concerning the group of the patient. In line with the principles of medical ethics, the patient did not have any information as to which group he belonged.
Having completed the checklist and entered the data in SPSS version 20 and based upon the goals and assumptions, descriptive statistics including tables, charts and distribution and central indexes were obtained and analytical analysis was carried out using appropriate methods such as independent T-test or non-parametrical methods were used to test the mean difference in various groups. To account for the changes observed in variables during different times, Repeated measure test was utilized.
Results
As many as 68 patients applying for elective surgery took part in this research. In the NAC group, there were 16 female (47%) and 18 male (53%) patients. In the NS group, there were 14 female (41%) and 20 male (59%) patients (P=0.713). The average age of the patients in NAC and NS groups was 44±12.4 and 44.3±10.9 years old respectively (p=0.137).
The average weight of the patients in NAC group was 65.8±6.4 kg, while this value for those in the NS group was 72.9±10.5 kg (P=0.214). 27 patients (79.4%) were in the NAC group and 32 (94.1%) were in ASA I normal saline group and the rest were in two groups of ASA II (p=0.283).
To study the para-clinical and hemodynamic parameters in various times, variance test with repeated measures was used. These values are presented in table 1.
Table 1. Values of kidney parameters in two groups before, 1 hour and 24 hours after operation
| Before operation | 1 hour after operation | 24 hours after operation | P-value | ||
| AST | NAC | 29.2±6.5 | 22.7±5.7 | 20.9±8.5 | P=0.0001*
F=13.75 |
| NS | 22.1±14.4 | 26.5±13.2 | 22.9±13.5 | ||
| ALT | NAC | 20.7±4 | 14.3±3 | 12±3.8 | P=0.0001*
F=27.55 |
| NS | 21.9±16.5 | 21.5±16 | 18.9±15.8 | ||
| LDH | NAC | 362±90.3 | 312.5±54 | 300.9±33.8 | P=0.0001*
F=19.41 |
| NS | 354.9±50.8 | 383.8±51 | 371.7±53.6 | ||
| PT | NAC | 11.8±0.2 | 13.9±5.3 | 12.7±0.5 | P=0.368
F=1.01 |
| NS | 11.9±0.5 | 12.4±1.1 | 11.7±0.2 | ||
As for measurement of heart beat, intergroup Wilkes lambda test with a value of F=8.193 and a significance level of p=0.0001 is indicative of the significant reduction of heartbeat in both groups. Intergroup analysis also showed a significant difference between groups (P=0.0001, F=6.49). Mauchly test was also achieved with a significance level of 0.000 which indicates the lack of variance error.
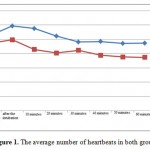 |
Figure 1: The average number of heartbeats in both groups
|
The intergroup Wilkes lambda test with a value of F=1.245 and a significance of P=0.323 shows that reduction of average diastolic blood pressure in both groups is not significant. Intergroup analysis also showed that there was no significant difference between groups (F=1.456 and P=0.174).
Once again, the intergroup test with a value of F=3.258 and a level of significance of P=0.014 showed that reduction of average systolic blood pressure in two groups is not significant. As the intergroup analysis showed, there is no significant difference between groups (F=1.716, P=0.096).
Concerning arterial oxygen pressure, intergroup Wilkes lambda test with a value of F=8.000 and a level of significance of P=0.464 showed that rise of the average arterial oxygen pressure in both groups is not significant. Intergroup analysis also showed a significant difference between the groups (P=0.003, F=2.985). Mauchly test was also gained with a significance level of 0.000 which indicated no variance error.
Discussion
The results of the present study showed that liver enzymes after operation in the NAC group are significantly less than the NS group. However, in terms of coagulating factors such as PT, APTT and INR, there was no statistically significant difference between the two groups. Concerning hemodynamic parameters, the number of heart beats and the level of arterial oxygen pressure in NAC group was significantly more than the NS group, but the difference between systolic or diastolic blood pressure of two groups was not significant.
In the case of toxicity with anesthetics, liver is affected more than any other body organ as it is a place where the inhaled medicines are metabolized. If there are no unusual issues in the history and examination of the patient, there is no need to study liver enzymes on a routine basis. Thus, it is not necessary to measure liver enzymes before operation and checking these enzymes before operation must be carried out based on any history of liver damages or results of physical examination. In such cases, first AST and ALT enzymes are measured (10, 11).
In a study whose results were published by Nishiyama et al., the level of ALT increased insignificantly among those patients who had undergone non-liver operations using Sevoflurane while the level of AST had remained constant (12). In a research conducted by Soma et al, Sevoflurane was prescribed for monkeys three hours a day, 3 days a week and for a period of 8 weeks (13). As the results indicated, repeated anesthesia with Sevoflurane resulted in a partial increase of AST, ALT and LDH. In this research, the liver enzyme returned to its normal level within a period of 4-8 weeks and there were no signs of liver histopathologic damage. Thus, they arrived at the conclusion that Sevoflurane had no significant influence on healthy people. In another research conducted by Wissing et al., the level of ALT and AST in kids who had undergone Desflurane 2 to 3% reduced insignificantly (14). The authors came to the conclusion that according to the available information, this reduction of liver enzymes cannot be described and justified. In the current research, the level of liver enzymes either decreased or remained constant which was in line with the above-said researches (12-14).
The basic reactions of liver in metabolism of medicines consist of 2 phases. P450 mono-oxidase and oxidase systems are responsible for phase 1 reactions which are called bio-transformation (15). This enzyme system is the main path of sevoflurane, isoflurane, enflurane and desflurane path. Of all these medicines, it is only sevoflurane that requires phase 2 reactions to discharge the final metabolic products (16).
In the study conducted by Nishiyama et al, liver performance enzymes were measured after anesthesia with sevoflurane and isoflurane (17). No significant rise was observed in liver enzymes within 24 hours in any of the groups. The highest rise in isoflurane group was recorded on the 7th day although this rise in the level of AST, ALT and LDH was not statistically significant. This research also studied coagulation factors such as PT, PTT, and INR. All these factors are synthesized in liver except for VIII factor (18, 19). According to the results of the study conducted by Nishiyama, the level of PT within 1 hour and 24 hours after operation had increased significantly, but the level of PTT remained within the normal range. In the current study, PT, PTT, and INR also remained within the normal range which was in line with this study.
Oxidative stress is the results of imbalance between free radicals of oxygen and internal anti-oxidant systems. N-acetyl cysteine is the most common external anti-oxidant which is used to deal with oxidative damages caused to tissue. The anti-oxidant influence of N-acetyl cysteine is due to its direct effects or the secondary effects caused by higher rates of Glutathione production. Its direct effect is reaction with hydroxyl radicals and deactivation of them. N-acetyl cysteine also prevents wasting glutathione and increases the levels of glutathione in liver. In an animal sample of acute kidney damage, glutathione could prevent Ischemic damages (20). In another study conducted by Misra et al in order to study the role of acetyl cysteine in preventing the Nephropathy caused by contrast material after cardiovascular actions, they arrived at the conclusion that using N-acetyl cysteine along with hydration with saline has positive clinical effects in preventing Nephropathy compared to when using saline alone (21). In the research conducted by Tepel et al, 88 patients with a history of acute kidney failure were divided into acetyl cysteine and control groups and coronary vessels angiography was carried out. The occurrence of Nephropathy caused by the contrast agent in N-acetyl cysteine group was 2%, while this percentage in the control group was 21% which is indicative of a significant difference between groups (22). In a similar research conducted by Diaz-Sandoval, 54 patients were studied. The dangerous factor studied was acute kidney failure. The results pointed to the fact that nephropathy of contrast agents was formed 45% in the control group and 8% in N-acetyl cysteine group which indicates the significant influence of this medicine (23).
All the inhaled medicines reduce the blood flow of liver veins in a dose-dependent manner. Based on the type of medicine selected, this reduction in liver blood flow during anesthesia and operation is 20 to 25%. The important causes of this reduction might be higher Sympathic tone or pressure on vena cava system as a result of higher pressure inside the chest cage during controlled ventilation. Reduction of liver flow usually takes place along with liver hypoxia (24, 25). The effects of isoflurane and sevoflurane on the total arterial liver flow (portal vein and hepatic artery) were measured. Sevoflurane can partially reduce portal blood flow, but increases hepatic artery flow. Thus, it will have effects similar to liver arterial flow on isoflurane (26).
In a hypoxic environment, hepatotoxicity of volatile anesthetics increases as the energy required by tissues and cells is not provided (27, 28). Particularly in hypoxic environments, halothanes cause more histopathologic damages than isoflurane in researches conducted on the liver of rats.
Conclusion
N-acetyl cysteine is an anti-oxidant medicine whose effects on the organs that dispose medicines such as kidney and liver have been repeatedly measured. In this research and after using isoflurane, this medicine could decrease liver enzymes significantly compared to control group. Seemingly, more researches and with a bigger sample are required to study the effects of such medicines. It is recommended to use other doses of this medicine in future studies.
References
- Kharasch ED. Adverse drug reactions with halogenated anesthetics. Clinical pharmacology and therapeutics. 2008;84(1):158-62. Epub 2008/05/30.
CrossRef - Turner GB, O’Rourke D, Scott GO, Beringer TR. Fatal hepatotoxicity after re-exposure to isoflurane: a case report and review of the literature. European journal of gastroenterology & hepatology. 2000;12(8):955-9. Epub 2000/08/25.
CrossRef - Reichle FM, Conzen PF. Halogenated inhalational anaesthetics. Best practice & research Clinical anaesthesiology. 2003;17(1):29-46. Epub 2003/05/20.
- Peiris LJ, Agrawal A, Morris JE, Basnyat PS. Isoflurane hepatitis-induced liver failure: a case report. Journal of clinical anesthesia. 2012;24(6):477-9. Epub 2012/06/05.
- Njoku DB, Shrestha S, Soloway R, Duray PR, Tsokos M, Abu-Asab MS, et al. Subcellular localization of trifluoroacetylated liver proteins in association with hepatitis following isoflurane. Anesthesiology. 2002;96(3):757-61. Epub 2002/03/02.
- Kelly GS. Clinical applications of N-acetylcysteine. Alternative medicine review : a journal of clinical therapeutic. 1998;3(2):114-27. Epub 1998/05/13.
- Dekhuijzen PN. Antioxidant properties of N-acetylcysteine: their relevance in relation to chronic obstructive pulmonary disease. The European respiratory journal : official journal of the European Society for Clinical Respiratory Physiology. 2004;23(4):629-36. Epub 2004/04/16.
- Sambo P, Amico D, Giacomelli R, Matucci-Cerinic M, Salsano F, Valentini G, et al. Intravenous N-acetylcysteine for treatment of Raynaud’s phenomenon secondary to systemic sclerosis: a pilot study. The Journal of rheumatology. 2001;28(10):2257-62. Epub 2001/10/24.
- Jepsen S, Herlevsen P, Knudsen P, Bud MI, Klausen NO. Antioxidant treatment with N-acetylcysteine during adult respiratory distress syndrome: a prospective, randomized, placebo-controlled study. Critical care medicine. 1992;20(7):918-23. Epub 1992/07/01.
- Martin J. Inhaled Anesthetics:Metabolism and Toxicity. In: Miller R, editor. Miller’s Anesthesia. Philadelphia: Chuchill Livingstone; 2010. p. 642-3.
CrossRef - Toker A, Girgin N, Turker G, Kutlay O. [Are preoperative routine laboratory tests necessary in minor and moderate surgical procedures?]. Dicle Med J. 2008;35:120-7.
- Nishiyama T, Yokoyama T, Hanaoka K. Effects of sevoflurane and isoflurane anesthesia on arterial ketone body ratio and liver function. Acta anaesthesiologica Scandinavica. 1999;43(3):347-51. Epub 1999/03/19.
CrossRef - Soma LR, Tierney WJ, Hogan GK, Satoh N. The effects of multiple administrations of sevoflurane to cynomolgus monkeys: clinical pathologic, hematologic, and pathologic study. Anesthesia and analgesia. 1995;81(2):347-52. Epub 1995/08/01.
- Wissing H, Kuhn I. The effect of desflurane on liver function markers in infants and children. Report of a study and a pertinent case report. Acta anaesthesiologica Scandinavica. 2000;44(9):1149-53. Epub 2000/10/12.
- Kharasch ED, Thummel KE. Identification of cytochrome P450 2E1 as the predominant enzyme catalyzing human liver microsomal defluorination of sevoflurane, isoflurane, and methoxyflurane. Anesthesiology. 1993;79(4):795-807. Epub 1993/10/01.
- Frink EJ, Jr. The hepatic effects of sevoflurane. Anesthesia and analgesia. 1995;81(6 Suppl):S46-50. Epub 1995/12/01.
- Nishiyama T, Yokoyama T, Hanaoka K. Liver function after sevoflurane or isoflurane anaesthesia in neurosurgical patients. Canadian journal of anaesthesia = Journal canadien d’anesthesie. 1998;45(8):753-6. Epub 1998/10/30.
- De Gasperi A, Corti A, Mazza E, Prosperi M, Amici O, Bettinelli L. Acute liver failure: managing coagulopathy and the bleeding diathesis. Transplantation proceedings. 2009;41(4):1256-9. Epub 2009/05/23.
- Tanaka KA, Key NS, Levy JH. Blood coagulation: hemostasis and thrombin regulation. Anesthesia and analgesia. 2009;108(5):1433-46. Epub 2009/04/18.
- Itoh Y, Yano T, Sendo T, Oishi R. Clinical and experimental evidence for prevention of acute renal failure induced by radiographic contrast media. Journal of pharmacological sciences. 2005;97(4):473-88. Epub 2005/04/12.
- Misra D, Leibowitz K, Gowda RM, Shapiro M, Khan IA. Role of N-acetylcysteine in prevention of contrast-induced nephropathy after cardiovascular procedures: a meta-analysis. Clinical cardiology. 2004;27(11):607-10. Epub 2004/11/26.
- Tepel M, van der Giet M, Schwarzfeld C, Laufer U, Liermann D, Zidek W. Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. The New England journal of medicine. 2000;343(3):180-4. Epub 2000/07/20.
- Diaz-Sandoval LJ, Kosowsky BD, Losordo DW. Acetylcysteine to prevent angiography-related renal tissue injury (the APART trial). The American journal of cardiology. 2002;89(3):356-8. Epub 2002/01/26.
- Frink EJ, Jr., Morgan SE, Coetzee A, Conzen PF, Brown BR, Jr. The effects of sevoflurane, halothane, enflurane, and isoflurane on hepatic blood flow and oxygenation in chronically instrumented greyhound dogs. Anesthesiology. 1992;76(1):85-90. Epub 1992/01/11.
- Conzen PF, Vollmar B, Habazettl H, Frink EJ, Peter K, Messmer K. Systemic and regional hemodynamics of isoflurane and sevoflurane in rats. Anesthesia and analgesia. 1992;74(1):79-88. Epub 1992/01/01.
- Bernard JM, Doursout MF, Wouters P, Hartley CJ, Merin RG, Chelly JE. Effects of sevoflurane and isoflurane on hepatic circulation in the chronically instrumented dog. Anesthesiology. 1992;77(3):541-5. Epub 1992/09/01.
- Pohorecki R, Howard BJ, Matsushita M, Stemmer PM, Becker GL, Landers DF. Isoflurane isomers differ in preservation of ATP in anoxic rat hepatocytes. The Journal of pharmacology and experimental therapeutics. 1994;268(2):625-8. Epub 1994/02/01.
- Howard BJ, Pohorecki R, Becker GL, Landers DF. Energy status in anoxic rat hepatocytes: effects of isoflurane, solution composition, and hypothermia. Liver transplantation and surgery : official publication of the American Association for the Study of Liver Diseases and the International Liver Transplantation Society. 1995;1(4):220-4. Epub 1995/07/01.

This work is licensed under a Creative Commons Attribution 4.0 International License.



