

Manuscript accepted on : 03 September 2016
Published online on: --
Plagiarism Check: Yes
Adenomyoma of the Small Intestine in a Child, A Case Report
Leila Hajimaghsoudi1, Ali Hashemi2, Koorosh Ahmadi3, Mahdi Foroughian4 and Mohsen Ebrahimi5*
1Department of Surgery, Alborz University of Medical Sciences, Karaj, Iran.
2Department of Pathology, Alborz University of Medical Sciences, Karaj, Iran.
3Department of Emergency Medicine, Alborz University of Medical Sciences, Karaj, Iran.
4Department of Emergency Medicine, Kerman University of Medical Sciences, Kerman, Iran.
5Department of Emergency Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
Corresponding Author E-mail: Ebrahimimn@mums.ac.ir
DOI : http://dx.doi.org/10.13005/bbra/2305

ABSTRACT: Adenomyoma is a tumor including components derived from glands and muscle. The main position of Adeomyoma occurrence is the stomach and the second most frequent location is the small bowel, usually in the periampullary area. and its occurrence in the small intestine distal to the duodenum is very rare. A 9 years old male patients admitted to the hospital with abdominal pain, nausea, and vomiting. The patient underwent surgery with acute appendicitis diagnosis. In addition to the inflammation of the appendix, a 3 cm nodule within 150 cm of ileocecal valve without any adhesion to the surrounding tissues was observed during the surgery. Our histopathological findings of this patients did not show goblet cells in all part of lesion. Adenomyom of ileum is rare disorder and the location of this lesion was not reported before.
KEYWORDS: Adenomyoma; Goblet cells; Ileum; Child
Download this article as:| Copy the following to cite this article: Hajimaghsoudi L, Hashemi A, Ahmadi K, Foroughian M, Ebrahimi M. Adenomyoma of the Small Intestine in a Child, A Case Report. Biotech Res Asia 2016;13(3). |
| Copy the following to cite this URL: Hajimaghsoudi L, Hashemi A, Ahmadi K, Foroughian M, Ebrahimi M. Adenomyoma of the Small Intestine in a Child, A Case Report. Biotech Res Asia 2016;13(3). Available from: https://www.biotech-asia.org/?p=16032 |
Introduction
Adenomyoma is a tumor including components derived from glands and muscle. [1] It is a type of complex and mixed tumor. In obstetrics and gynecology contexts, it is a form of adenomyosis that forms a mass or growth around the tissue of the inner uterus. Most cases of adenomyosis are non-symptomatic. However, it may present with dysmenorrhea and pelvic pain. In case of juvenile cystic adenomyoma, laparoscopic enucleation results in a statistically and clinically significant reduction in dysmenorrhea, ease in any chronic pelvic pain and low risk of recurrence. [2]
Adenomyoma of the gastrointestinal tract is a benign tumor-like condition characterized histologically by abnormal glandular formations lined by mucin-secreting columnar epithelium and surrounded by bundles of smooth muscles. [3-5] Magnus Alsleben, in 1903 was the first one who described adenomyomas with stomach localization. [6] It also has several other names such as myoepithelial hamartoma [7-11], adenomyomatous hamartoma [12, 13], and foregut choristoma [14]. It arises from pancreatic metaplasia or a displaced pancreatic anlage during embryogenesis. [15]
The main position of Adeomyoma occurrence is the stomach [1] and the second most frequent location is the small bowel, usually in the periampullary area. [16] and its occurrence in the small intestine distal to the duodenum is very rare. [17] The most common clinical presentations of adenomyoma in the small bowel are intussusception and intestinal or biliary obstruction, which is depend on the location of the lesions. [5, 7, 12, 13, 18] Although most cases refer to adults, they may also appear at any age [19] and it also has been seen in children. [20] Herein we try report a 9 years old patient who suffer from adenomyoma in the small intestine distal and near to ileocecal valve.
Case Presentation
A 9 years old male patients admitted to the Bahonar hospital, Karaj with abdominal pain, nausea, and vomiting. Due to the investigation, the patient did not have any history of a particular disease in past. Lower abdominal pain and tenderness with leukocytosis and urine turbidity, and small renal calculus in the lower calyx of left kidney and lymph node with diameter up to 0.7 mm were our other findings obtained from this patient.
The patient underwent surgery with acute appendicitis diagnosis. In addition to the inflammation of the appendix, a 3 cm nodule within 150 cm of ileocecal valve without any adhesion to the surrounding tissues was observed during the surgery. Histopathologic examination showed that the nodule lesion made up of pancreatic cystic ducts with smooth muscle tissue. Pancreatic glandular components were not observed in this tissue. These pathological findings consistent with adenomyoma in this area. (Figure 1 and 2)
The young patient discharged after the surgery and standard diet with a normal postoperative course.
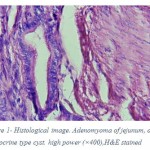 |
Figure 1: Histological image. Adenomyoma of jejunum, dilated exocrine type cyst. high power (×400),H&E stained.
|
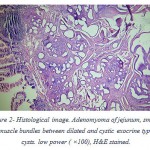 |
Figure 2: Histological image. Adenomyoma of jejunum, smooth muscle bundles between dilated and cystic exocrine type cysts. low power ( ×100), H&E stained.
|
Discution
Adenomyoma of the gastrointestinal (GI) tract is a rare lesion and only a small number of them occur in the small bowel distal to the duodenum. [12] Symptoms of adenomyoma of the GI tract depend on the location of the lesion and patient’s age. Adenomyoma of the periampullary area usually presents with biliary obstruction (obstructive jaundice) or abdominal pain. [21] Jejunal and ileal adenomyoma of pediatric patients usually presents with intussusceptions. [22] In adult patients, intussusception is an infrequent complication, with many reported cases having been incidentally detected during surgery for other diseases or during autopsy. Several cases presenting with GI bleeding (melena) have been reported. [10, 23]
The pathogenesis of adenomyoma of the GI tract is generally considered to be either a form of hamartoma or a pancreatic heterotopia, although it is not fully understood. The term ‘hamartoma’ means an excessive but focal overgrowth of cells or tissues native to the organ in which it occurs. The term ‘heterotopia’ means microscopically normal cells or tissues existing in an abnormal location. The existence of goblet and Paneth cells in the glandular element of the present case seemed to suggest that the lesion was a true hamartoma. [17]
Their localization at the small intestine of children is extremely rare (Table 1). Intussusception is the most common complication of adenomyoma of the small intestine, as was the case with our patient. Thus far, of the 13 reported cases of adenomyoma in children, only two did not cause intussusception: in one case, intestinal obstruction preceded, and the other concerned an incidental finding. [3, 19, 22] It is notable that this disorder also has been seen in higher ages and not shown here. These reports shows that adenomyoma do not have any relation to the patients age. Based on comparison of other reports it can be seen that this lesion at ileum is more common in male children.
Table 1: Summery of reported adenomyoma located in ileum
| Study | Age/Sex | Size (cm) | Location |
| Roseman et al [22] | 2 Days/F | NA | Ileum, submucosa |
| Kim et al [14] | 7 Years/M | 4 | Ileum, submucosa |
| Gal et al [12] | 9 Months/M | 1.2 | Ileum, submucosa, and muscularis |
| Serour et al [24] | 4 Years/M | 2 | Ileum, Submucosa |
| Chan and Roche [3] | 5 Months/F | 0.8 | Ileum, Submucosa |
| Schwartz et al [25] | 8 Months/M | 2 | Ileum |
| Lamaki et al [26] | 1 Year/M | 1 | Ileum |
| Gonzalvez et al [8] | 2 Years/M | 2 | Ileum |
| Yamagami et al [11] | 4 Months/M | NA | Ileum |
| Mouravas et al [19] | 1.5 Year/M | 1 | Ileum |
| Park et al [13] | 7 Months/M | 1.2 | Ileum |
| Temiz et al [27] | 11 Years/M | 1.5 | Ileum |
| Bak et al [28] | 11 Months/F | 1 | Ileum |
| Current Report | 9 Years/M | 3 | Ileum |
| NA: Not Available | |||
Adenomyoma of the small intestine is formed by glandular structure lined by columnar epithelium and surrounded by smooth muscle. Cystic changes often occur in the ducts. Adenomyoma and ectopic pancreatic tissue can be seen in a variety of pathological changes. Acinar and pancreatic islet tissue usually can be seen in ectopic pancreatic tissue. [13] Sever gastrointestinal bleeding is rare symptom of both these disorders. These nodules are often a random finding during abdominal surgery. Anatomically, adenomyom location at distal duodenum is very rare. Only 26 percent of all reported adenomyoms have been located at small intestine. These nodules can be manifested as an intussusception in children. The size of nodules can be varying from 0.6 to 6 cm. [15]
Based on pathological studies, the goblet cells observed only in 5 of 22 patients with small intestine adenomyom. [17] Our histopathological findings of this patients did not show goblet cells in all part of lesion.
Abdominal pain can be mentioned as a common presenting symptom in these patients. Hamartoma polyps in peutz jegher syndrome and/or metastatic adenocarcinoma can be mentioned as pathological differential diagnosis of this disorder. The absence of Desmoplastic stroma and also lack of cellular atypia are two important criteria for differentiation of malignant cases. [18, 23]
In summary, adenomyom of ileum is rare disorder and the location of this lesion was not reported before. On the other hand, goblet cells were not separated in all part of the nodule base on histopathological findings.
References
- Vandelli, A., et al., Adenomyoma of the stomach. Surgical endoscopy, 1993. 7(3): p. 185-187.
CrossRef - Takeuchi, H., et al., Diagnosis, laparoscopic management, and histopathologic findings of juvenile cystic adenomyoma: a review of nine cases. Fertility and sterility, 2010. 94(3): p. 862-868.
CrossRef - Chan, Y.-F. and D. Roche, Adenomyoma of the small intestine in children. Journal of pediatric surgery, 1994. 29(12): p. 1611-1612.
CrossRef - Chapple, C., S. Muller, and J. Newman, Gastric adenocarcinoma associated with adenomyoma of the stomach. Postgraduate medical journal, 1988. 64(756): p. 801-803.
CrossRef - Lee, J.S., et al., Adenomyoma of the small intestine in an adult: a rare cause of intussusception. Journal of gastroenterology, 2002. 37(7): p. 556-559.
CrossRef - E., M.-A., Adenomyome de pylorus. Archiv für Pathologische Anatomie und Physiologie und für Klinische Medicin, 1903. 173(1): p. 137-155.
- Clarke, B., Myoepithelial hamartoma of the gastrointestinal tract: a report of eight cases with comment concerning genesis and nomenclature. Arch Pathol, 1940. 30: p. 143-152.
- Gonzalvez, J., et al., Myoepithelial hamartoma of the ileum: a rare cause of intestinal intussusception in children. European journal of pediatric surgery, 1995. 5(05): p. 303-304.
CrossRef - Hizawa, K., et al., Jejunal myoepithelial hamartoma associated with Gardner’s syndrome: a case report. Endoscopy, 1996. 28(8): p. S1-S78.
CrossRef - Tanaka, N., et al., Myoepithelial hamartoma of the small bowel: report of a case. Surgery today, 1996. 26(12): p. 1010-1013.
CrossRef - Yamagami, T., K. Tokiwa, and N. Iwai, Myoepithelial hamartoma of the ileum causing intussusception in an infant. Pediatric surgery international, 1997. 12(2-3): p. 206-207.
CrossRef - Gal, R., Z. Kolkow, and M. Nobel, Adenomyomatous hamartoma of the small intestine: a rare cause of intussusception in an adult. American Journal of Gastroenterology, 1986. 81(12).
- Park, H.S., et al., Adenomyoma of the small intestine: report of two cases and review of the literature. Pathology international, 2003. 53(2): p. 111-114.
CrossRef - Kim, C.J., G.Y. Choe, and J.G. Chi, Foregut choristoma of the ileum,(adenomyoma)-a case report. Pediatric Pathology, 1990. 10(5): p. 799-805.
CrossRef - Yu, H.-C., et al., Adenomyoma of the jejunum—a rare cause of gastrointestinal bleeding. Journal of the Chinese Medical Association, 2008. 71(2): p. 96-99.
CrossRef - Ryan, A., et al., Myoepithelial hamartoma of the duodenal wall. Virchows Archiv, 1998. 432(2): p. 191-194.
CrossRef - Takahashi, Y., et al., Adenomyoma with goblet and Paneth cells of the ileum. Pathology-Research and Practice, 2006. 202(7): p. 549-553.
CrossRef - Bedirli, A., et al., Periampullary adenomyoma: report of two cases. Surgery today, 2002. 32(11): p. 1016-1018.
CrossRef - Mouravas, V., et al., Adenomyoma of the small intestine in children: a rare cause of intussusception. The Turkish journal of pediatrics, 2003. 45: p. 345-347.
- Bush Jr, W.H., D.G. Hall, and B.H. Ward, Adenomyosis of the Gastric Antrum in Children 1. Radiology, 1974. 111(1): p. 179-181.
CrossRef - Handra-Luca, A., et al., Adenomyoma and adenomyomatous hyperplasia of the Vaterian system: clinical, pathological, and new immunohistochemical features of 13 cases. Modern pathology, 2003. 16(6): p. 530-536.
CrossRef - Rosenmann, E., C. Maayan, and O. Lernau, Leiomyomatous hamartosis with congenital jejunoileal atresia. Israel journal of medical sciences, 1980. 16(11): p. 775.
- Ghartimagar, D., Ileal adenomyoma in an elderly female. Research, 2014.
- Serour, F., et al., Adenomyoma of the small bowel: a rare cause of intussusception in childhood. Journal of pediatric gastroenterology and nutrition, 1994. 18(2): p. 247-249.
CrossRef - SCHWARTZ, S.I. and H.M. RADWIN, Myoepithelial hamartoma of the ileum causing intussusception. AMA archives of surgery, 1958. 77(1): p. 102-104.
CrossRef - Lamki, N., et al., Adenomyomatous hamartoma causing ileoileal intussusception in a young child. Clinical imaging, 1993. 17(3): p. 183-185.
CrossRef - Temiz, A. and H.A. Kahya, Ileal Adenomyoma: Extremely Rare Cause of Intussusception. Journal of Academic Emergency Medicine, 2015. 14(4): p. 207.
- Bak, Y.-J., et al., Adenomyoma of the small intestine a rare pathological lead point for intussusception in an infant. SpringerPlus, 2014. 3(1): p. 1-4.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.



