

Manuscript accepted on :
Published online on: --
Evaluation of Dysmorphic Features in Intellectual Disability
Minakshi Vashist, Ritu Yadav, Kirti Grow and Shiksha Sharma
Department of Genetics, Maharshi Dayanand University, Rohtak. Haryana, India.
Corresponding Author E-mail: ritugenetics@gmail.com
DOI : http://dx.doi.org/ http://dx.doi.org/10.13005/bbra/1068

ABSTRACT:
Five hundred intellectually disabled persons of different districts of Haryana state have been recorded and analyzed in the present study. Detailed questionnaire of dysmorphic features has been developed for different level of intellectual disability. More than twenty five dysmorphic features were studied and different level of intellectual disability was determined by Seguin board test. In the present study, 70% intellectually disabled person revealed presence of one or the other dysmorphic features and in 30% of intellectually disabled persons no dysmorphic features could be observed. Presence or absence of unusual features helps in investigation to steer further diagnosis studies. The use of more specific and diagnostic approaches will lead to better clarification of the etiology. An important implication of finding a cause and knowing the aetiology of person with intellectual disability is that their families can be educated about the long term issues such as life span and progression of disease, decision about child bearing and antenatal monitoring of subsequent pregnancies.
KEYWORDS:
Dysmorphic features; Intellectual disability; Etiology; Level of severity.
| Copy the following to cite this article: Vashist M, Yadav R, Grow K, Sharma S. Evaluation of Dysmorphic Features in Intellectual Disability. Biosci Biotech Res Asia 2012;9(2) |
| Copy the following to cite this URL: Vashist M, Yadav R, Grow K, Sharma S. Evaluation of Dysmorphic Features in Intellectual Disability. Biosci Biotech Res Asia 2012;9(2). Available from: https://www.biotech-asia.org/? p=10138 |
Introduction
Intellectual disability is one of the most frequent handicaps among children and can be a serious and life long disability placing heavy demands on the society and the health system [1, 2].
Association of Intellectual disability and congenital malformation has long been recognized and necessary component of evaluation of child with idiopathic Intellectual disability is a comprehensive dysmorphologic examination [3].
Analysis of dysmorphic features or development of milestones can be used for assessment of intellectually disabled child rather than a diagnosis tool or service because no cross tables could be gathered. Different studies of dysmorphological examination were performed in such a different way or the data was presented in such a different manner that pooling of results was not feasible or useful. However, there were few parameters of similar results for a general dysmorphological evaluation. The first is the presence within the families or other family members with intellectual disability. Two or more dysmorphic features were found with high (39.4% – 44.5%) to very high (55.0%- 81.9%) frequency in large groups of persons with intellectual disability [4]. This was reported in a number of studies [5- 9]. The median number of families in which relatives with intellectual disability were present was 15.0% (range 7.5–46%). The presence of dysmorphic features and positive family history of intellectual disability indicate that 30-50% of undiagnosed cases may fall to moderate and severe category [10]. However, it was generally not stated to which extent the family was surveyed for intellectual disability nor to which extent it was reported in the publication.
Cytogenetic analysis at a 400-500-band resolution is the standard investigation for suspected chromosomal rearrangement. The range of chromosomal abnormalities on routine cytogenetic analysis is 2.93% to 11.6%, with median of 3.7% [11]. Chromosome abnormalities in 4 out of 10 cases of intellectual disability had no dysmorphic features [12]. Chromosomal analysis of child with mild developmental delay, who does not have dysmorphic features, is still somewhat controversial, as the majority of persons will have normal results. The most common effect of a chromosome abnormality is cognitive impairment, but it is also frequently associated with defects of heart formation and dysmorphic features [13]. Presence or absence of unusual dysmorphic features may help in investigation of intellectually disabled persons. A need for more standardization of reporting dysmorphological examinations is always emphasized.
Method of Study
Dysmorphic features of all intellectually disabled persons were subjected to detailed analysis. These were diagnosed with the help of clinicians. In the present study, five hundred intellectually disabled persons were studied for presence of one or the other dysmorphic features. Level of cognitive functioning (IQ) was determined using Seguin form board test. Level of intellectual disability was divided into four different classes. The classification was done as per WHO system of classification [14]. Thirty dysmorphic features of each person have been recorded with help of ‘Questionnaire’. Abnormal dysmorphic features or dysmorphic features were divided into three regions i.e. Head & face region, hand region and feet region. Photographs of various features were taken with the consent of parents and guardians. Variability in dysmorphic features of intellectual disabled person was statistically analysed.
Result
In the present study, 70% intellectually disabled person revealed presence of one or the other dysmorphic features. There were 30% of intellectually disabled persons in whom no dysmorphic features could be observed. Persons of moderate intellectual disability group revealed dysmorphic features in 39% cases, whereas mild and severe group revealed 14% and 17% cases respectively.
Table 1: Percentage frequency of intellectual disabled persons showing dysmorphic features.
| IQ level | Dysmorphic features | Normal dysmorphic features |
| Mild | 14.0
|
13.6 |
| Moderate | 39.0
|
15.0 |
| Severe | 17.0
|
1.4 |
Head and face region
Four types of head anomalies were found in the intellectually disabled person i.e. microcephaly, macrocephaly, hydrocephaly and brachycephaly. Macrocephaly and microcephaly were present in equal frequency (1.6%), whereas 1.2% persons showed hydrocephalus and 34% persons showed brachycephaly. Constantly open mouth was prominent feature of intellectually disabled persons & it was observed in 65% persons. Flattened nasal bridge was present in 36.2% of intellectually disabled persons. Other abnormal features revealed variable frequency such as upturned nares in 12.8%, epicanthal fold in 34%, slanting palpebral fissure in 46%, flat occipital region in 36%, fissured lips in 55%, and protruded tongue in 30.4% of intellectual disabled persons. Mottled skin with reddish rim was found in 23.2% persons. There were 9% cases of intellectual disability with abnormal enamel genesis (Fig. 1)
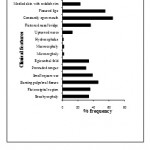 |
Figure 1: Clinical features of (Head and face) of intellectual disabled persons.
|
Hand region
Short Stubby hand was most prominent feature seen in intellectually disabled persons. Single transverse palm crease was found in 22% of cases. Presence of hyper extensibility of fingers was seen in 6.2% persons and long, thin tapered fingers in 3.4% cases. Partial syndactyly in 2nd and 3rd fingers and polydactyl were found in 2.4% of intellectually disabled persons.
Feet region
Fifty eight percent cases of intellectual disability showed short 4th or 5th metatarsal in feet region. Most recognizable features in feet was deep crease between 1st and 2nd toes, it was present in 48% of intellectually disabled persons. Wide gap between 1 and 2nd toes was found in 36 % cases. Broad and large big toe was seen in 14.2 % persons. Polydactyly of toes and partial syndactyly of 2nd and 3rd toes was found in 1.6% and 0.4% of intellectually disabled persons respectively (Fig. 2).
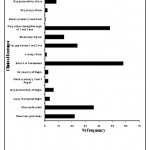 |
Figure 1: Clinical features of (Head and face) of intellectual disabled persons.
|
Discussion
The physical finding results in the patient were the most important factors in determining whether or not a diagnosis could be made. The diagnosis was more significant when patient has an unusual appearance and numbers of features are more. The presence of a major malformation did not increase the diagnostic rate. Diagnosis was established in 1 of 30 persons on the basis of physical examination [15]. In another study, pathogenesis diagnosis identified in 80% of all persons. Half of the persons were diagnosed by history and physical examination alone [16].Global development delays help in making diagnosis in 63.3%. History and physical examination alone acted as diagnostic tool in 18.4% [17]. In a study of 99 children, diagnosis was made by history and physical examination alone in 38.6% [4].
In another study, the frequency of two or more dysmorphic features was from high 39.4% to very high 55.0% [15, 17]. Importance of physical examination, including pediatric, neurological, and dysmorphological examinations was reported and found essential for the diagnosis in 62% and contributory in 79% [10]. Limited number of studies was reported on the percentage of persons with abnormal physical features in a population. However presence of abnormal features was reported in 55%, 44.5%, and 39.4% 81.9% intellectually disabled persons [10, 15, 17-20]. It was expected that the physical examination would be the most important determinant of diagnostic success. In the present study, 70% cases of intellectual disability revealed dysmorphic features. Although the number of persons with major malformation in present study was small and the data support the observation that the presence of additional major malformations does not increase the probability of a diagnosis. It was noted that the likelihood of making a diagnosis was not influenced by the severity of the intellectual disability. This contrasts often expressed opinion that the yield of genetic diagnoses is greater in children with severe intellectual disability; where as in the present study 5.7% cases of severe intellectual disability were having major associated disorders like cerebral palsy, microcephaly, and epilepsy. There was report of association of microcephaly with increasing severity of intellectual disability [21]. The utility of a dysmorphological examination was difficult to evaluate. The main reason was that very limited number of studies is reported on the specific result of such examination. Numerical results on the resulting diagnostic yield cannot be derived from these studies. Association of intellectual disability and congenital malformation has long been recognized and presence or absence of unusual features may help in investigation to steer further diagnosis studies. The use of more specific and diagnostic approaches will lead to better clarification of the etiology.
The consensus conference recognized that the need of dysmorphic evaluation for cases of intellectual disability has not been addressed systematically in the literature. In the present study large differences were found in dysmorphical features therefore, it can be suggested that taking a good clinical history and performing a detailed physical examination by a trained specialist remains the basis of every aetiological study in children with intellectual disability.
Conclusion
Dysmorphic features are very important in diagnosis of intellectually disabled persons in society. This screening may led to early detection of moderately and severely retarded children. It may also help in establishment of various screening programmes and rehabilitation centers.
Acknowledgment
The authors are grateful for all the individuals for their cooperation in giving useful information for filling up the questionnaires. M.D. University Rohtak, University grants commission (F-36-162/2009(SR), CSIR (09/382(0128)/2008-EMR-1) and ICMR (5/4-4/13/M/2006- NCD.1), New Delhi are gratefully acknowledged for giving fellowships to research scholars and providing funds for carrying out the research work.
References
- Pollak, M.: Handicapped children. In: Text book of developmental paediatrics. (Pollak M, ed). Edinburgh, United Kingdom: Churchill Livingstone, 1993; pp 459-504.
- Swaiman, K. F.: Intellectual disability. In: Pediatric Neurology: “Principles and Practice” (Swaiman KF, ed). St. Louis, Missouri: Mosby Yr Book, 1994; pp 133-146.
- Schaefer, G. B., Bodensteiner, J. B. Evaluation of the child with idiopathic intellectual disability. Pediatr. Clin. North. Am., 1992; 39: 929-943.
- Shevell, M. I., Majnemer, A., Rosenbaum, P., Abrahamowicz, M. Etiologic yield of subspecialist’s evaluation of young children with global developmental delay. J. Pediatr., 2000; 136: 593–598.
- Sinclair, S. Etiological factors in intellectual disability: A study of 470 cases. Ind. Pediatr., 1972; 9: 391−396.
- Matilainen, R., Airaksinen, E., Mononen, T., Launiala, K., Kaariainen, R. A population-based study on the causes of mild and severe intellectual disability. Acta. Paediatr., 1995; 84: 261−266.
- Stromme, P. Aetiology in severe and mild intellectual disability: A population based study Norwegian children. Dev. Med. child. Neurol., 2000; 42 (2): 76-86.
- Tan, B. S., Law, H. Y., Zhao, Y., Yoon, C. S. DNA testing for fragile X syndrome in 255 males from special schools in Singapore. Ann. Acad. Med. Singapore., 2000; 29: 207-212.
- Karnebeek, V. C. D. M., Scheper, F. Y., Abeling, N. G.: Aetiology of intellectual disability or borderline cognitive delay in 281 children referred to a tertiary care center: a prospective study. In: Intellectual disability: Diagnostic Studies on Aetiology (van Karnebeek C. D. M., ed), Ph.D. Thesis submitted to Department of Pediatrics/Emma Children’s Hospital and Department of Clinical Genetics, Academic Medical Centre, University of Amsterdam, Amsterdam, Netherlands, 2002.,75-108.
- Fryns, J.P., Volcke, P.H., Haspeslagh, M., Beusen, L., Van, DenBerghe H. A genetic diagnostic survey in an institutionalized population of 262 moderately mentally retarded patients. J. Ment. Defic. Res., 1990; 34: 29-40.
- Shevell, M. I., Ashwal, S., Donley, D. Practice parameter: Evaluation of child with global developmental delay. Report of Quality standards subcommittee of the American Academy of Neurology and The Practice committee of the child Neurology society. Neuro., 2003; 60: 367-80.
- Graham, S.M., Selikowitz, M. Chromosome testing in children with developmental delay in whom the aetiology is not evident clinically. J. Paediatr. Child. Health., 1993; 29: 360-362.
- Barber, J. C. Directly transmitted unbalanced chromosome abnormalities and euchromatic variants. J. Med. Genet., 2005; 42: 609-629.
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders. Clinical Description and Diagnostic Guidelines. Geneva: World Health Organization. 1993; DOI: 10.2277/0521861810.
- Hunter, A. G. Outcome of the routine assessment of patients with intellectual disability in a genetics clinic. Am. Med. Genet., 2000; 90: 60-68.
- Battaglia, A., Carey, J. C. Diagnostic evaluation of developmental delay/ intellectual disability: an overview. Am. J. Med. Genet., 2003; 117: 3-14.
- Majnemer, A., Shevell, M. I. Diagnostic yield of the neurological assessment of the developmentally delayed child. J. Pediatr., 1995; 127: 193-99.
- Ohdo, S., Sonoda, T., Ohba, K., Hayakawa, K. Etiologic and pathogenetic study of intellectual disability with multiple congenital anomalies. Acta. pediatr. Jpn., 1992; 34: 144-150.
- Battaglia, A., Bianchini, E., Carey, J. C. Diagnostic yield of the comprehensive assessment of developmental delay/intellectual disability in an institute of child neuropsychiatry. Am. J. Med. Genet., 1999; 82: 60-66.
- Saul, R. A., Stevenson, R. E., Schroer, R. J. Congenital anomalies in individuals with intellectual disability proc greenwood. Genet. Crt., 1996; 15: 160.
- Fernell, E. Mild intellectual disability in schoolchildren in a Swedish suburban municipality: prevalence and diagnostic aspects. Acta. Paediatr., 1996; 85: 584-8.

This work is licensed under a Creative Commons Attribution 4.0 International License.



