

Manuscript accepted on : June 29, 2011
Published online on: 28-06-2011
Role of Calcium Channel Blockers in Inducing Gingival Enlargement - A Cross Sectional Study
Zameera A. Naik and Anjana Bagewadi
Department of Oral Medicine and Radiology, KlE VK Institute of Dental Sciences, KLE University, Belgaum India.
ABSTRACT: Background Calcium channel blockers (CCB) are the widely prescribed drugs for the management of hypertension. Gingival enlargement (GE) due to calcium channel blockers (CCB) accounts for a prevalence rate of 14.7%-83%. Literature reveals that the most frequently encountered CCB causing GE is nifedipine being 83%, and the least common is amlodipine being 3.3%. Amlodipine prescription is increasing in the recent years, attributed to its high patient compliance and cost effectiveness. The study was conducted with an aim to determine the association between GE and the use of different Calcium channel blockers and with an objective to assess the status of gingiva in patients on CCB, as well as to assess the relationship between dosage and duration of intake of CCB on the status of GE. Material and Methods The present study included 30 hypertensive subjects on calcium channel blockers and 30 healthy controls who were not on any of the drugs causing gingival enlargement. Written consent was obtained and history recorded for all the study subjects, Oral hygiene was assessed by Green and Vermillion index, gingival condition by Loe and Sillness index and the gingival enlargement was recorded using the Ingles index. Results 20(66%) subjects out of 30 had gingival enlargement among whom 12(40%) subjects had Grade II GE and 5(16%) had Grade III GE. This when compared to controls was statistically significant with p value of < 0.001. Conclusion Slightest of the local factors trigger the gingival response to the drugs causing gingival enlargement. GE provides new niches for growth of microrganisms, resulting in tooth loss. Clinicians should and must pay attention to patients oral hygiene prior to prescription of CCB and stress on need of regular dental visits.
KEYWORDS: Gingival enlargement; calcium channel blockers; gingivitis; duration
Download this article as:| Copy the following to cite this article: Naik Z. A, Bagewadi A. Role of Calcium Channel Blockers in Inducing Gingival Enlargement - A Cross Sectional Study. Biosci Biotech Res Asia 2011;8(1) |
| Copy the following to cite this URL: Naik Z. A, Bagewadi A. Role of Calcium Channel Blockers in Inducing Gingival Enlargement - A Cross Sectional Study. Biosci Biotech Res Asia 2011;8(1). Available from: https://www.biotech-asia.org/?p=9339 |
Introduction
Rapid advances in the field of technology, has lead to early diagnosis, treatment and prevention of diseases, at the same time there is also a rise in incidence of stress induced health problems.
As per the Global Burden of disease, hypertension is the major contributing factor for growing rate of cardiovascular diseases in India.
Hypertension being the most prevailing stress related disorder prevails in India with a rate of 24.9%1. Hypertension is treated by various groups of drugs and one among them are the calcium channel blockers (CCB). These CCB are well documented as a cause of GE in these patients. Till date nefidipine induced GE has prevalence rate of 83%2,3,4.
Amlodipine, one of the third generation dihydropyridine is the most commonly prescribed CCB in the recent years due to its effectiveness and increased patient compliance in terms of single dose and cost5. Amlodipine has side effects like constipation, drowsiness, of concern to the dentist is the gingival enlargement caused by it which is comparatively less prevalent. Literature reports few studies and cases regarding amlodipine induced gingival enlargement having a prevalence rate of 3.3%6,7,8,9,16,17.
As per Jorgensen et al (1997)9, there was no significant evidence of GE following use of amlodipine in 150 cardiac subjects examined by him and amlodipine was suggested to be a viable alternative to nefidipine. Seymour RA (1994)6 was first to document a case of amlodipine induced gingival enlargement.
In the light of above information, this study was conducted to determine the type of CCB causing GE, so that these patients are counseled to maintain good oral hygiene or drug substitution would be advised in consultation with the physician, and thereby improving the gingival health.
Materials and Methods
The study included 30 study subjects & 30 control subjects both being age and sex matched, reporting as outpatients to the Department of Oral Medicine and Radiology at our Institute. Subjects taking CCB as antihypertensives for atleast 6 months and having atleast 12 natural teeth and subjects with no periodontal treatment within the previous 6 months were included in the study. However patients on polymedication for hypertension as well as other systemic diseases, patients unwilling to participate and patients on other drugs associated with GE were excluded.
A written consent was obtained from all the study subjects, and the demographic as well as medical history regarding hypertension in terms of duration, type of medication and dose in mg was noted. Ethical clearance from the Institutional Review Board was obtained. History of oral hygiene was recorded in terms of brushing habit, which revealed whether the subject brushed using brush or finger, with paste or abrasive, frequency and method.
Oral hygiene was assessed by Green and Vermillion index, gingival condition using Loe and Sillness index and gingival enlargement by Ingles index10.Gingival enlargement was measured using periodontal probe placing it perpendicular to the gingiva labially or buccally. (Fig 1)
 |
Figure 1: showing measurement of GE using periodontal probe.
|
Statistical Analysis
The study parameters were tabulated and subjected for analysis using student‘t’ test, Chi-Square test. The intergroup comparison (between study and control groups) was done using ANOVA test.
Results and Observations
The study subjects ranged from 36-68 years with mean of 50.53±9 and 30 control subjects ranged from 32-63 years with mean of 49.37±8 (Table 1). The study comprised of 25(83%) females and 5(17%) males affirming the higher prevalence of hypertension among females, both groups being age and sex matched.
Table 1: Distribution of age of study and control subjects.
| Groups | Mild | Moderate | Severe | X12 and p value |
| Study subjects | 6 | 20 | — | 3.2 and 0.073 NS |
| Control subjects | 13 | 14 | 1 |
NS : Non significant
Distinctively almost all the subjects i.e 28(93%) in our study were taking amlodipine for more than 6 months with exception of one each on nefidipine and felodipine. This clearly revealed higher prescription of amlodipine.
Further 24 patients were on less than 5mg of amlodipine and 4 patients on greater than 5mgm.
As per the duration, 20 patients were on amlodipine for less than 5 years and 10 patients for greater than 5 years.
Brushing technique was more or less similar in both the study and control subjects, where maximum subjects used horizontal brushing method. In the present study, fair oral hygiene was present in 16(53%) study subjects and 20 (66%) had moderate gingivitis which was not significantly different from the controls(Table2).
Table 2: Distribution of type of gingivitis amongst the study and control groups.
| Groups | Mild | Moderate | Severe | X12 and p value |
| Study subjects | 6 | 20 | — | 3.2 and 0.073 NS |
| Control subjects | 13 | 14 | 1 |
NS : Non significant
Regarding GE, 20(66%) subjects in study group had GE among which 12(40%) subjects had Grade II GE, 5(16%) had Grade III and 3(10%) had Grade I GE, as compared to controls where none had Grade II GE, which was statistically significant with p value < 0.001. (Graph I, Table 3)
Table 3: subjects showing different grades of GE in study and control groups.
| Groups | Grade 0 | Grade I | Grade II | Grade III | X12 and p value |
| Study subjects | 10 | 3 | 12 | 5 | |
| Control subjects | 11 | 19 | 0
|
0 | 28.6 and <0.001
Sig |
Sig: Significant
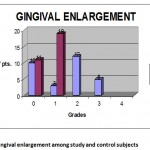 |
Graph 1: Gingival enlargement among study and control subjects.
|
10(42%) patients taking amlodipine less than 5 mg had Grade II GE and 4(17%) had Grade III GE, whereas 2(50%) patients taking greater than 5 mg had Grade II and 1(25%) had grade III GE(Graph II), suggesting that dose does not affect the severity of GE as the differences were statistically insignificant.
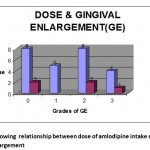 |
Graph 2: showing relationship between dose of amlodipine intake and gingival enlargement.
|
8(40%) patients taking amlodipine for duration less than 5 yrs , had Grade II GE and 4(40%) patients taking amlodipine for duration greater than 5 yrs, had Grade II GE, revealing lack of significant correlation between duration of intake of drug and GE.(Graph III, Table 4)
Table 4: Correlation between duration of CCB intake and gingival enlargement.
| Duration | Gingival enlargement | X12 and p value | |||
| Grade 0 | Grade I | Grade II | Grade III | ||
| ≤ 5 years | 6 | 3 | 8 | 3 | 0.018 and >0.05
NS |
| ≥ 5 years | 4 | – | 4 | 2 | |
NS : Non significant
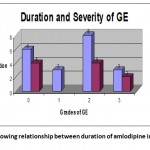 |
Graph 3: showing relationship between duration of amlodipine intake and GE.
|
Discussion
In the present study, the study subjects had a mean age of 50.5years which is similar to reports of Seymour RA et al (1994)6 ,Barclay (1992)3 and Amit Kumar et al(2010)17 who reported cases between 35-66years with hypertension but in contrast to study by Jorgensen G M(1997)9 who had patients in age range of 33-87 years which could be due to differing prevalence of hypertension among Indians, most common being the third decade.
Higher prevalence of hypertension among the females was observed, in the present study which is similar to that reported by Seymour RA et al (1994)6, Amit Kumar et al (2010)17 where all the patients affected were females, but in contrast to Barclay (1992)3 where 90% of males had reported.
Maximum subjects were on amlodipine which is due to its long duration of action and increased patient compliance as evaluated in a community survey1 and is similar to all the patients on amlodipine as reported in different case series7,8,16,17.
Fair oral hygiene was observed with moderate gingivitis which was in compliance with fair to poor oral hygiene as previously reported 9,17,18. Gingival enlargement increases in presence of poor oral hygiene and pre-existing gingival inflammation. Inflammation develops due to direct toxic effects of drug in GCF leading to upregulation of cytokines such as TGFβ1 promoting tissue overgrowth13,15. However it is also stated that individual susceptibility to develop fibrogenic response to the CCB is also variable. On the contrary Barclay et al3 and Jorgensen9 reported no relationship between gingival changes and plaque scores in their studies. Few authors have reported that evidence exists wherein oral hygiene procedures have reduced extent of GE and prevented its occurrence 11,12.
Regarding GE, maximum study subjects had Grade II GE which is in accordance to that reported by Lafzi (2006)13 who identified a patient with severe GE taking 10 mg amlodipine for 2 months ,Seymour RA (1994)6, Abirmani K etal (2004)8 ,Vishaka(2007)16 and Amit Kumar et al(2010)17 ,but contrast to Jorgensen(1997)9 who reported a prevalence of 3.3% of GE in 150 cardiac subjects on amlodipine(Graph I). This variation could be attributed to dosage variation, different population groups studied, different oral hygiene practices followed and varying individual susceptibility to GE.
Further dosage, duration of drug intake did not have any significant effect on severity of GE, which holds right for the fact that, patients on 5mgm of amlodipine for 6 months did not show GE9 when compared to patient on amlodipine only for 2 months had remarkable GE13, suggesting GE due to CCB to be multifactorial.
Our study subjects were referred to Department of Periodontology where they were subjected to periodontal therapy based on severity of GE. Mild to moderate GE subjects underwent scaling followed by root planning and curettage. Severe enlargement subjects were referred to their physicians and drug substitution was advised followed by surgical intervention.
GE provides susceptible sites for growth of microorganisms, reduces effectiveness of brushing, resulting in periodontitis. By the year 2025, it is estimated that 213.5 million people would be affected by HTN, with an expected increase in prescription of CCB. GE gets exacerbated in the presence of local factors.
Hence the general physicians should and must pay attention to patients oral hygiene while prescribing CCB and inform them regarding GE associated with these drugs. The oral physicians should emphasize on educating patients taking CCB to maintain good oral hygiene thus preventing GE, provided in cases where oral hygiene methods fail, drug substitution should be advised after consultation with the patient’s physician.
References
- Dr Shyamal Das, Kalyan Sanyal, Arindam Basu: Study of urban community survery in India: growing trend of high prevalence of hypertension in a developing country. Int J Med Sci, 2005,2: 70-78.
- Harel raviv: Nefidipine induced gingival hyperplasia. Triplo, 1995:79:715-22
- Barclay S, Thomason JM: The incidence and severity of nefidipine-induced gingival overgrowth. J of Clin Perio, 1992:19:311-314
- Edmundo B Nery, et al: Prevalence of Nefidipine induced gingival hyperplasia. J Perio, 1995:66:572-578
- Valcarcel; R.Jimenez; V.Hernandez; R. Aristegui; A. Gil : Efficacy and safety of amlodipine: Clin Drug Invest, 2006;26(3);125-133.
- Seymour RA, Ellis JS, Thomason JM et al : Amlodipine induced gingival overgrowth. J Clin Periodontol, 1994:21:281-283
- Roger Smith (Letter): Gingival enlargement in a patient medicated with amlodipine. Br Dent J ,1993:175:279
- K Abirmani, S Padmanabhan, V Sivakumar, (Letter): Amlodipine induced gingival hyperplasia. Indian J of Nephrology, 2004: 14: 72.
- Jorgensen GM: Prevalence of Amlodipine related gingival hyperplasia. J Perio, 1997:68:676-678
- Ingles E, Rossmann JA, Caffene R: New clinical index for drug induced gingival overgrowth. Quintessence Int. 1999; 30;467-473..
- Sholmo Barak, Issac S Engelberg and Jehuda Hiss: Gingival Hyperplasia caused by Nefidipine: J Perio, 1987, 58,9,639-642.
- Hanock RH, Swan RH: Nefidipine induced gingival overgrowth, Report of a case treated by controlling plaque. J Clin Perio, 1992,19,12-14.
- Lafzi A, Ramim M, Mohammadali M: Amlodipine induced gingival hyperplasia. J Oral med & Patho, 2006:11:480-482.
- Seymour RA : Calcium channel blockers and gingival overgrowth. Br Dent J, 1991:170:376.
- Ellis JS,et al: Gingival sequestration of amlodipine and amlodipine induced gingival growth(letter) Lancet, 1993:341:1102-1103.
- Vishaka Grover, Anoop Kapoor, CM Marya: Amlodipine induced Gingival Hyperplasia. J Oral Health Comm Dent, 2007;1(1);19-22.
- Amit Kumar S, Debabrata K, Prasanta B, Asit Kumar P: Management of amlodipine induced gingival enlargement: Series of three cases. J Indian Society of Periodontology, 2010 Vol 14; 4;279-281

This work is licensed under a Creative Commons Attribution 4.0 International License.



