

Manuscript accepted on : 21 February 2017
Published online on: --
Plagiarism Check: Yes
Yasir Hassan Elhassan, Salman Y. Guraya and Hamdi Almaramhy
College of Medicine, Taibah University Almadinah Almunawwarah Saudi Arabia.
Corresponding Author E-mail: salmanguraya@gmail.com
DOI : http://dx.doi.org/10.13005/bbra/2430

ABSTRACT: Perianal abscess is a common surgical emergency that is often treated by junior surgical trainees. This study aims to report the prevalence, clinical features, predisposing factors, and the outcome of surgical treatment of perianal abscess with particular attention to fistula in ano.The medical records of all consecutive patients admitted through emergency room and surgical clinics, from 2013 to 2015, in a single Saudi hospital were reviewed. The records of patients diagnosed with and treated for perianal abscess and fistula in ano were further reviewed for the pre-defined variables. of a total of 3618 patients, 198 (18.2%) had perianal abscess with a mean age of 35.9 years. The body mass index of the study cohort ranged from 16.5 to 39.7 with a mean of 32. As many as 141 (71%) patients had healed wounds after primary incision and drainage while 40 (20.2%) developed recurrent perianal abscess. Anal pain was the most common complaint noted in all 198 (100%) patients, followed by fever in 99 (50%). Forty (20.2 %; 32 men and 8 women) patients developed perianal fistula in ano. Forty six (23%) patients had predisposing risk factors including diabetes mellitus, hypertension, and Crohn’s disease. Diabetes mellitus was the most common disease that was complicated by perianal abscess in both genders.The reported prevalence of perianal abscess and the outcome of surgical treatment is in accordance with the published data. Common health problems such as diabetes mellitus, obesity, and hypertension predispose to perianal abscess and fistula in ano. Both the recurrence of abscess and the need for readmission are preventable if disease is adequately treated during initial intervention.
KEYWORDS: Diabetes mellitus; Fistula in ano;Crohn’s disease;Obesity; Perianal abscess; Prevalence
Download this article as:| Copy the following to cite this article: Elhassan Y. H, Guraya S. Y, Almaramhy H. The Prevalence, Risk factors and outcome of Surgical Treatment of Acute Perianal Abscess from A Single Saudi Hospital. Biosci Biotech Res Asia 2017;14(1). |
| Copy the following to cite this URL: Elhassan Y. H, Guraya S. Y, Almaramhy H. The Prevalence, Risk factors and outcome of Surgical Treatment of Acute Perianal Abscess from A Single Saudi Hospital. Biosci Biotech Res Asia 2017;14(1). Available from: https://www.biotech-asia.org/?p=22107 |
Introduction
Perianal abscess is a benign but common clinical condition that may cause substantial discomfort to the suffering patients and carries significant burden on healthcare services.1,2 Perianal abscess develops when crypt glands, about 8-10 glands located at the dentate line in a circumferential manner, are blocked by inspissated debris that results in unabated bacterial overgrowth.3 Subsequently, acute-phase suppurative process ensues that expands towards the tissues of least resistance, the commonest being ischiorectal and supralevator spaces.4 The peak incidence of perianal abscess has been reported to be in the 3rd or 4th decade of life and it is two or three times more common in men than women.5 Although the reason for this increased preponderance in men is uncertain, however, an increased local androgen conversion in anal glands has been proposed as a possible mechanism.6 The predisposing factors that lead to the development of perianal abscess include malignancy particularly colorectal cancer,7,8,9 trauma (10), diabetes mellitus,11 tuberculosis,12 leukemia, obesity,13,14 HIV15 and inflammatory bowel disease.16,17 Interestingly, colorectal cancer can metastasize internally by developing coloenteric fistulas18,19 as well as into the perianal region in the form of perianal fistula.20
Incision and drainage of perianal abscesses are common surgical emergency procedures that are primarily performed by junior surgical trainees. Literature has shown that about 40% patients develop a fistula in ano after primary incision and drainage of perianal abscess.15,21 As perianal abscess frequently co-exists with fistula in ano, failure to identify and treat the internal opening at the time of primary operation may result in chronic fistulation and recurrent abscesses.21 Such recurrent abscesses potentially increase the risk of anal incontinence.22 Nevertheless, published work fails to provide clear evidence about which patients go on to develop a fistula. Some researchers have postulated that positive cultures from perianal abscesses with gut related organisms enhance the likelihood of an underlying fistula,23 while others denied the predictive value of this hypothesis.24,25
This retrospective study explored the prevalence, presenting features, predisposing risk factors, and the outcome of the surgical management for perianal abscess. A further analysis of fistula in ano, resulting from the surgical therapies or that were missed during the primary incision and drainage is also described.
Materials and Methods
In this retrospective study, the medical records of all consecutive patients admitted through the surgical clinics and emergency room of the Meeqat General Hospital (MGH) Almadinah Almunawwarah Saudi Arabia, from August 2013 to August 2015, presenting with perianal abscess were reviewed. The MGH is the only healthcare facility in the city of Almadinah Almunawwarah that caters the acute infectious diseases such as perianal abscess and diabetic foot. All patients with perianal abscess were subjected to incision and drainage and were discharged after uneventful recovery. The medical records of patients with perianal abscess were scrutinized for demographic analysis, presenting features, single or multiple nature of perianal abscess, superficial or deep, duration of disease, comorbidities, outcome of surgery whether cured or recurred, and the prevalence of perianal fistula in ano recorded in this cohort. The data was transferred on Excel sheets and further analysis was performed to record the frequency charts, histograms and the resulting incidence of fistula in ano. An official ethical approval was obtained from the Ethical Review Committee of the college of medicine Taibah University for conducting this research.
Results
During the study period, of a total of 3,618 patients, 198 (18.2%) were diagnosed with perianal abscess. There were 159 (80%) men and 39 (20%) women. The age range of men was 11 to 76 years with an average of 37.8 years and that of women was 15 to 67 years with a mean age of 34.5 years. Overall, the body mass index (BMI) for the entire cohort ranged from 16.5 to 39.7 with a mean of 32. Anal pain was the most common presenting complaint of perianal abscess noted in all 198 (100%) patients, followed by fever in 99 (50%) (Figure 1). The incidence of anal pain and perianal swelling were equal in both genders; whereas fever, constipation and discharge were more common in women.
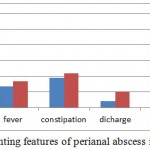 |
Figure 1: The presenting features of perianal abscess in this study (N=198)
|
The duration of symptoms of perianal abscess at the time of presentation is shown in Figure 2. Women had longer duration than the male counterparts.
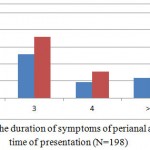 |
Figure 2: The duration of symptoms of perianal abscess at the time of presentation (N=198)
|
Note; X axis denotes the duration of symptoms of perianal abscess in days
Forty six (23%) patients with perianal abscess had comorbid conditions such as diabetes mellitus (40 patients), hypertension (3), and Crohn’s disease (3) as shown in Figure 3. Diabetes mellitus was the most common disease that was complicated by perianal abscess in both genders. Another group of 10 (19%) patients had some kind of pelvic surgery before developing perianal abscess. 171 (86%), 137 men and 34 women, had superficial and 27 (14%), 20 men and 7 women, were found to have deep seated perianal abscesses.
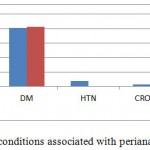 |
Figure 3: Comorbid conditions associated with perianal abscess (N=198)
|
One hundred and sixty five (83%) patients were found to have a single perianal abscess, while 12 (6%) had more than one (multiple) abscesses. The medical record of the rest of 21 patients could not identify the number of perianal abscesses.
One hundred and forty one (71%) had healed wounds after the surgical drainage of perianal abscess, 40 (33 men and 7 women) patients had recurrent perianal abscess that necessitated second operation, and another 40 (32 men and 8 women) patients developed perianal fistula in ano; the prevalence of fistula in ano being 20.2% from 198 patients with perianal abscess and 1.105% from the study cohort of 3,618 patients. All three patients with Crohn’s disease had fistula in ano, while 27 (65%) with diabetes mellitus developed fistula in ano. Figure 4 illustrates the association of comorbidities with and without perianal fistula in his study.
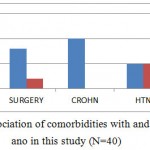 |
Figure 4: The association of comorbidities with and without fistula in ano in this study (N=40)
|
Note; DM stands for diabetes mellitus, HTN hypertension
Twenty eight patients presented more than two days after the development of fistula in ano; whereas four patients presented within two days after developing fistula in ano (Figure 5).
 |
Figure 5: Correlation between the duration and presentation of fistula in ano (N=40)
|
Discussion
In this study, the prevalence of perianal abscess is more common in men than women. Several other studies have reported this male preponderance. 26,13,27 Additionally, the mean age of 34.5 years in this study cohort is similar with the mean age of 39.8 years reported by Ulug et al.28 Similar mean age has been reported by other studies.29,30 The reported incidence of 18.2% in this study is slightly higher than 16.1% from a study by Adamo et al.13
Anal pain and perianal swelling dominated the presenting features of perianal abscess in the current study. Although the prevalence of anal pain and perianal swelling were equal in both genders, fever, constipation and discharge were more common in women. This perhaps reflects the shyness due to cultural and religious barriers prevailing in the region. Other studies have also reported the same clinical characteristics of perianal abscess of anal pain, discharge, swelling, and fever.31,32
In our study, diabetes mellitus was the most common disease that was complicated by perianal abscess in both genders. Several studies have argued that although the exact pathogenesis is not clear, Crohn’s disease, diabetes, and obesity increase the risk for perianal abscess as well as the risk for recurrence.33,34,35 Hyperglycemia is associated with impaired microcirculation due to atherosclerosis, deranged immune response, and sub optimal fibroblast function.36 All these abnormalities predispose to soft tissue infection including perianal abscess. A study has demonstrated that perianal abscesses predispose to the development of type 2 diabetes mellitus within five years of the primary diagnosis.37 This may be due to the change in lifestyle that the patient with perianal abscess has to adopt.
In our study, all three patients with Crohn’s disease presented with perianal abscess and later developed fistula in ano. The incidence of perianal disease in Crohn’s disease has been reported be in the range of 3·8 % to 80 %.38,39 This variation is partly related to different defining criteria. Perianal abscesses occur in 23–62 % of patients with Crohn’s disease and are usually associated with a concurrent fistula in ano.40“The more complex the fistula tract the higher the incidence of abscess formation”.41 Research has shown that 20–36 % of perianal disease precedes the manifestations of intestinal component of Crohn’s disease.42,43 In the current disease, the presence of fistula in ano might have been missed at the time of primary operation for perianal abscess and this might be a lesson for the junior trainee surgeons to careful look for an internal opening for fistula in ano while draining the perianal abscess.
The range of BMI in this study cohort ranged from 16.5 to 39.7 with a mean of 32. Currently, obesity is one of the most challenging health problem that predisposes to several health problems such as endocrine, metabolic, and cardiovascular disorders of diabetes, hypertension and coronary heart disease.44 Obesity impairs wound healing and predisposes to soft tissue infections.45 However, the exact mechanism leading to impaired and delayed wound healing is unknown. A study by Schwandner has shown that obesity was a negative predictor of successful outcome after surgery for complex fistula in ano.46 This study inferred that obesity was an independent risk factor predicting failure after surgery for complex fistula in ano. This could be due to the increased prevalence of co-morbidities associated with obesity as compared to non-obese patients.
This study showed that 141 (71%) patients had healed wounds after the primary incision and drainage of perianal abscess, while 40 (20.2%) patients developed perianal fistula in ano. A study showed that the incidence of fistula in ano among the different populations in the European Union ranged from 1.04 per 10,000/year in Spain to 2.32 per 10,000/year in Italy with a confidence interval from 1.20 up to 2.80.47 This is consistent with the prevalence of fistula in ano in our study. However, we could not find an accurate estimated rate of incidence of fistula in ano from Saudi Arabia. Read et al. reported a 34% incidence of fistula in ano following the surgical drainage of anorectal abscess with a 95% confidence interval of 30-38%.35 The surgical team involved in the study under consideration deliberate performed exploration of every patient with anorectal abscess to identify internal opening of the concurrent fistula in ano. Another study showed a fistula rate of 26.4% with a 95% confidence interval 19.4-33.4%.48 However, the surgeons in this study did not advocate probing and deliberate exploration of the abscess cavity.
The described approaches to dealing with perianal abscess at the time of primary operation by probe or by simple incision and drainage generates interest in exploring more evidence-based studies to reach a general consensus among the treating surgeons. In the present study, the cavity of perianal abscess was not probed for internal opening of a co-existing fistula in ano as the majority of procedures were performed by junior surgical residents and, per se, probing was not practiced in the MGH. Despite diverging approaches, the incidence of fistula in ano remains in a similar range across different regions of the world. In our study, 28 patients presented more than two days after the development of fistula in ano, while four patients presented within two days after developing fistula in ano. All three patients with Crohn’s disease had fistula in ano; whereas 27 (65%) with diabetes mellitus developed fistula in ano.
There is no agreed surgical strategy whether to probe for the internal opening of co-existing fistula in ano. Currently, the outcome measures for both surgical approaches, probing and non-probing, have shown similar rate of success but a unified surgical approach will help guide the surgical trainees to follow a standard protocol while dealing with perianal abscess. Such measures can help reduce the rates of readmissions for recurrences and for fistula in ano that can significantly curtail the burden on the financial and economic resources of health institutions.
Conclusion
The prevalence of perianal abscess and fistula in ano in Almadinah Almunawwarah is similar to the reported literature. Diabetes mellitus, previous pelvic surgery, obesity, Crohn’s disease, and hypertension have been identified as the key predisposing factors for perianal abscess and fistula in ano. In view of significant burden on health resources, the governmental policy makers and stakeholders are urged to raise the public awareness program for preventing and controlling the common health problems that lead to associated co-morbidities such as perianal abscess and fistula in ano.
Authors’ contribution
YHE conceived the idea, collected data and performed initial data analysis. SYG performed further data analysis, conducted literature review and wrote initial and final draft of the manuscript. HHM revised the data analysis and revised the manuscript. All authors agreed and approved the final manuscript.
Conflicts of interests
No conflicts declared.
Ethical approval
A formal ethical approval was obtained by the Institution’s ethical review committee for conducting this research and an informed consent was taken from all participants in this study. There are no concerns about data sharing in this research.
Acknowledgement
The authors appreciate the support provided by Dr. Kamran Yousaf, surgical specialist at MGH, in data collection.
References
- Liu C. K., Liu C. P., Leung C. H., Sun F. J. Clinical and microbiological analysis of adult perianal abscess. Journal of Microbiology, Immunology and Infection. 2011;44(3):204-8.
CrossRef - George B. D. Anal and perianal disorders. Medicine. 2007;35(3):147-52.
CrossRef - Sud A., Khan A. Benign anal conditions haemorrhoids fissures perianal abscess fistula-in-ano and pilonidal sinus. Surgery (Oxford). 2014;32(8):421-6.
CrossRef - Malik A., Hall D., Devaney R., Sylvester H., Yalamarthi S. The impact of specialist experience in the surgical management of perianal abscesses. International Journal of Surgery. 2011;9(6):475-7.
CrossRef - Rickard M. J. Anal abscesses and fistulas. ANZ journal of surgery. 2005;75(1‐2):64-72.
CrossRef - Lunniss P., Jenkins P., Besser G., Perry L., Phillips R. Gender differences in incidence of idiopathic fistula-in-ano are not explained by circulating sex hormones. International journal of colorectal disease. 1995;10(1):25-8.
CrossRef - Eltinay O. F., Guraya S. Y. Colorectal carcinoma: Clinico-pathological pattern and outcome of surgical management. Saudi Journal of Gastroenterology. 2006;12(2):83.
CrossRef - Guraya S. Y., Eltinay O. E. Higher prevalence in young population and rightward shift of colorectal carcinoma. Saudi medical journal. 2006;27(9):1391-3.
- Guraya S. Y. The Non Surgical Management of Colonoscopic Perforations: Worthwhile To Take Risk? Journal of Taibah University Medical Sciences. 2007;2(1–2):23-9.
CrossRef - Steele S. R., Kumar R., Feingold D. L., Rafferty J. L., Buie W. D. Practice parameters for the management of perianal abscess and fistula-in-ano. Diseases of the colon & rectum. 2011;54(12):1465-74.
CrossRef - Guraya S. Y. The association of type 2 diabetes mellitus and the risk of colorectal cancer a meta analysis and systematic review.World J Gastroenterol. 2015;21(19):6026-6031.
- Kraemer M., Gill S. S., Seow-Choen F. Tuberculous anal sepsis. Diseases of the colon & rectum. 2000;43(11):1589-91.
CrossRef - Adamo K., Sandblom G., Brännström F., Strigård K. Prevalence and recurrence rate of perianal abscess—a population-based study, Sweden 1997–2009. International journal of colorectal disease. 2016:1-5.
CrossRef - Ibrahim S. A., Samy M. A., Saleh A. O. L., Ahmed G. S., Matter M. K. Obesity among Egyptian Adults with Short Stature “Arabic abstracts”. Journal of Taibah University Medical Sciences. 2010;5(2):A6.
CrossRef - Hamadani A., Haigh P. I., Liu I. L. A., Abbas M. A. Who is at risk for developing chronic anal fistula or recurrent anal sepsis after initial perianal abscess? Diseases of the colon & rectum. 2009;52(2):217-21.
CrossRef - Bornstein J. E., Steinhagen R. M. History of Crohn’s Disease. Crohn’s Disease: Springer. 2015;1-13.
- Alrubaiy L., Rikaby I., Hutchings H. A., Williams J. G. Can the inflammatory bowel disease biologics registry lead to improved quality of care? Journal of Taibah University Medical Sciences. 2015;10(3):373-5.
CrossRef - Guraya S. Y., Murshid K. R. Malignant duodenocolic fistula. Various therapeutic surgical modalities. Saudi medical journal. 2004;25(8):1111-4.
- Guraya S. Y., Khairy G. A., Ghallab A., Al-Saigh A. Carcinoid tumors of the appendix. Our experience in a university hospital. Saudi medical journal. 2005;26(3):434-7.
- Shwaartz C., Munger J. A., Deliz J. R., Bornstein J. E., Gorfine S. R., Chessin D. B., et al. Fistula-Associated Anorectal Cancer in the Setting of Crohn’s Disease. Diseases of the Colon & Rectum. 2016;59(12):1168-73.
CrossRef - Knoefel W. T., Hosch S. B., Hoyer B., rn o, Izbicki J. R. The initial approach to anorectal abscesses: fistulotomy is safe and reduces the chance of recurrences. Digestive surgery. 2000;17(3):274-8.
CrossRef - Quah H., Tang C., Eu K., Chan S., Samuel M. Meta-analysis of randomized clinical trials comparing drainage alone vs primary sphincter-cutting procedures for anorectal abscess–fistula. International journal of colorectal disease. 2006;21(6):602-9.
CrossRef - Grace R., Harper I., Thompson R. Anorectal sepsis: Microbiology in relation to fistula‐in‐ano. British journal of surgery. 1982;69(7):401-3.
CrossRef - Fielding M., Berry A. Management of perianal sepsis in a district general hospital. Journal of the Royal College of Surgeons of Edinburgh. 1992;37(4):232-4.
- Narayanan A., Sundararaman S., Varadhan L., Rajput R., Reay-Jones N., Gupta V. The value of microbiological analysis of pus swabs in perianal abscess. Have they stood the test of time and antibiotic usage? International Surgery Journal. 2015;2(2):175-8.
CrossRef - Lunniss P., Phillips R. Surgical assessment of acute anorectal sepsis is a better predictor of fistula than microbiological analysis. British journal of surgery. 1994;81(3):368-9.
CrossRef - Akkapulu N., Dere Ö., Zaim G., Soy H. E. A., Özmen T., Doğrul A. B. A retrospective analysis of 93 cases with anorectal abscess in a rural state hospital. Turkish Journal of Surgery. Ulusal cerrahi dergisi. 2015;31(1):5.
CrossRef - Ulug M., Gedik E., Girgin S., Celen M. K., Ayaz C. The evaluation of bacteriology in perianal abscesses of 81 adult patients. Brazilian Journal of Infectious Diseases. 2010;14(3):225-9.
CrossRef - Toyonaga T., Matsushima M., Tanaka Y., Shimojima Y., Matsumura N., Kannyama H., et al. Microbiological analysis and endoanal ultrasonography for diagnosis of anal fistula in acute anorectal sepsis. International journal of colorectal disease. 2007;22(2):209-13.
CrossRef - Albright J. B., Pidala M. J., Cali J. R., Snyder M. J., Voloyiannis T., Bailey H. R. MRSA-related perianal abscesses an underrecognized disease entity. Diseases of the colon & rectum. 2007;50(7):996-1003.
CrossRef - George B. D. Anal and perianal disorders. Medicine. 2011;39(2):84-9.
CrossRef - Pego-Reigosa R., Brañas-Fernández F., Garcia-Porrua C., Gonzalez-Gay M. Sciatic nerve palsy as presenting sign of a perianal abscess. Joint bone spine. 2003;70(1):85-6.
CrossRef - Wei P. L., Keller J. J., Kuo L. J., Lin H. C. Increased risk of diabetes following perianal abscess a population-based follow-up study. International journal of colorectal disease. 2013;28(2):235-40.
CrossRef - Yoshino H., Kawakami K., Yoshino G., Sawada K. Case of anal fistula with Fournier’s gangrene in an obese type 2 diabetes mellitus patient. Journal of Diabetes Investigation. 2015.
- Read D. R., Abcarian H. A prospective survey of 474 patients with anorectal abscess. Diseases of the colon & rectum. 1979;22(8):566-8.
CrossRef - Casqueiro J., Casqueiro J., Alves C. Infections in patients with diabetes mellitus: A review of pathogenesis. Indian journal of endocrinology and metabolism. 2012;16(7):27.
CrossRef - Ommer A., Herold A., Berg E., Fürst A., Sailer M., Schiedeck T. German S3 guideline: anal abscess. International journal of colorectal disease. 2012;27(6):831-7.
CrossRef - Schwartz D. A., Loftus E. V., Tremaine W. J., Panaccione R., Harmsen W. S., Zinsmeister A. R., et al. The natural history of fistulizing Crohn’s disease in Olmsted County.Minnesota. Gastroenterology. 2002;122(4):875-80.
CrossRef - Lewis R. T., Maron D. J. Anorectal Crohn’s disease. Surgical Clinics of North America. 2010;90(1):83-97.
CrossRef - Solomon M. Fistulae and abscesses in symptomatic perianal Crohn’s disease. International journal of colorectal disease. 1996;11(5):222-6.
CrossRef - Scott M. H. J., Northover J. M. Evaluation of surgery for perianal Crohn’s fistulas. Diseases of the colon & rectum. 1996;39(9):1039-43.
CrossRef - Fry R. D., Shemesh E., Kodner I., Timmcke A. Techniques and results in the management of anal and perianal Crohn’s disease. Surgery, gynecology & obstetrics. 1989;168(1):42-8.
CrossRef - Singh B., Jewell D., George B. Perianal Crohn’s disease. British journal of surgery. 2004;91(7):801-14.
CrossRef - Yano T., Asano M., Matsuda Y., Kawakami K., Nakai K., Nonaka M. Prognostic factors for recurrence following the initial drainage of an anorectal abscess. International journal of colorectal disease. 2010;25(12):1495-8.
CrossRef - Pierpont Y. N., Dinh T. P., Salas R. E., Johnson E. L., Wright T. G., Robson M. C., et al. Obesity and surgical wound healing: a current review. ISRN obesity. 2014;2014.
- Schwandner O. Obesity is a negative predictor of success after surgery for complex anal fistula. BMC gastroenterology. 2011;11(1):61.
CrossRef - Zanotti C., Martinez-Puente C., Pascual I., Pascual M., Herreros D., García-Olmo D. An assessment of the incidence of fistula-in-ano in four countries of the European Union. International journal of colorectal disease. 2007;22(12):1459-62.
CrossRef - Isbister W. Fistula in ano: a surgical audit. International journal of colorectal disease. 1995;10(2):94-6.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.



