

Manuscript accepted on : 24 February 2016
Published online on: 09-04-2016
Farzad Poorgholami1, Marzieh Kargar Jahromi2, Navid Kalani3 and Razieh Parniyan4*
1Reaserch Center for Non-Communicable Diseases , Jahrom University of Medical Sciences, Jahrom, Iran 2Community Health Nursing, Faculty of Nursing & Para-Medicine, Jahrom University of Medical Sciences, Jahrom, Iran 3Medical Ethics Research Center, Jahrom University of Medical Sciences, Jahrom, Iran 4Medical Surgical Nursing, Faculty of Nursing and Para-Medicine, Jahrom University of Medical Sciences, Jahrom, Iran. Correspomding Authors E-mail: r_parniyan22@yahoo.com
DOI : http://dx.doi.org/10.13005/bbra/2052

ABSTRACT: End-stage renal disease (ESRD) is an irreversible clinical condition.These patients have many problems during treatment with dialysis such as physical, mental, and socioeconomic problem To assessthe influence of educational interventions based on the continuous care model on the quality of life of hemodialysis patients. The present study is a controlled clinical trial.The study population consisted of the entire patients with advanced chronic kidney failure who were undergoing hemodialysis at hemodialysis ward of OstadMotahri Hospital in 2014-2015. The subjects were selected based on the purposeful sampling method. Based on the findings of the study the researchers set the final size at 25 subjects in each group. In the end, 50 hemodialysis patients were randomly assigned to the control and the experimental groups. The quality of life of the subjects in both groups was evaluated using Ferrans and Powers Quality of Life Index Dialysis Version before and after the intervention. Independent sample t-test showed that there were no significant differences between the two groups in all quality of life subtypes before intervention(P=0.6). But after the intervention there were Significant differences between the two groups in the quality of life subtypes questionnaire. Thequality of life aspects of the intervention group were higher than the controls (P<0001). This strategy can also be recommended for increasing QOL in patients suffering other chronic diseases.
KEYWORDS: Educational Interventions; Continuous Care Model; Quality of Life; Hemodialysis Patients
Download this article as:| Copy the following to cite this article: Poorgholami F, Jahromi M. K, Kalani N, Parniyan R. The Influence of Educational Interventions based on the Continuous Care Model on the Quality of Life of Hemodialysis Patients. Biosci Biotech Res Asia 2016;13(1) |
| Copy the following to cite this URL: Poorgholami F, Jahromi M. K, Kalani N, Parniyan R. The Influence of Educational Interventions based on the Continuous Care Model on the Quality of Life of Hemodialysis Patients. Biosci Biotech Res Asia 2016;13(1). Available from: https://www.biotech-asia.org/?p=7676 |
Introduction
End-stage renal disease (ESRD) isan irreversible clinical condition. These patients will treatment with replacement therapies. (Sayin, Mutluay, and Sindel, 2007; Georg &Neilson, 2008)
Since kidney transplantation has numerous limitations;more renal failure patient must to cope withdialysis. Dialysis can improve health related quality of life (QOL), but these patients have many problems during treatment with dialysis such as physical, mental, and socioeconomic problem. All of the previous problem impact their health related QOL (Ebad, Sodani, Faghihi, &Hosseinpoor, 2009; Poorgholami, Javadpour,Saadatmand, & KargarJahromi, 2016).
The previous studies shown that quality of life of patients with chronic renal failureunder hemodialysis had been. In addition, the majority of these patients suffer frommuch psychological distress thatthese problems impact on their quality of life (SabetghadamPoorgholami et al., 2016).
The scientific research on hemodialysis patient shown by increasing in QOL they still have many stressful variable and upset.(Barone, Martin-Watson, &Barone, 2004).Therefore, QOL has been importance issue in practical research studies (Marci, & Donald, 1996)
Quality of life is important because it show outcome of patient (Shu-fen, & Chu, 2006).If we assess the QOL of patients with chronic diseases it help us that diagnosis the disease better and quickly. In the next step we can evaluate the prognosis of received medical care and supported treatment (Rahimi, Ahmadi, &Gholyaf, 2006).Thus we can determine the best procedure and method for improving the QOL of these patients (Salari, MehdizadehSEbadi, Aslani, &Naderi, 2009)
One of the important nursing roll in the clinical environment is considered to be patient training (including public awareness of hospital roles, cause and symptoms of diseases, treatment and self-care, etc.) (Noohi&Pouraboli, 2009). This role has been explained by the American Nursing Association (ANA) Standards of Clinical Nursing Practice (KargarJahromi, Javadpour, Taheri, &Poorgholami, 2016).
Education of these patient has many benefits, including decrease healthcare costs, and helping patients to achieve greater independence and self-sufficiency (NajafiMehri, Vahedparast, Hafezi, Saghafi, Farsi, &Vahabi, 2008).
We can use effectively from nursing models and theories for improvement of QOL. Using models improve caring regimen activity. Ahmadi in 2001 introduced the continuous care model. It is a native nursing care model, used to establish and maintain a dynamic, interactive, and mutual relationship between the nurse, the patient, and the patient’s family, so that the QOL of the patients may be improved(Salari, Mehdizadeh, Ebadi, Aslani, & Naderi,2009; Rahimi, Ahmadi, &Gholyaf ,2008). The aim of this article was the influence of educational interventions based on the continuous care model on the quality of life of hemodialysis patients.
Method
Study Design
The present study is a controlled clinical trialthat aims to improve the quality of life of hemodialysis patients.
Study Setting and Sample
After the study plan had been authorized by the ethics committee of Jahrom University of Medical Sciences, the study was conducted in the hemodialysis ward of OstadMotahri Hospital of Jahrom for 4 months, beginning in September 2015 and ending in December 2015.
The participantwere the entire patients with end stage renal failure who were undergoing hemodialysis at hemodialysis ward of OstadMotahri Hospital in 2014-2015. The subjects were selected based on the purposeful sampling method. Based on the findings of the study of Poorgholami (Poorgholami, Javadpour, Saadatmand, &Kargar Jahromi,2016) and considering an alpha of 5% and a beta of 90% and using Altman’s nomogram, sample size was set at 26 subjects in each group. However, considering the possibility of a 15% sample loss, the researchers set the final size at 30 subjects in each group. In the end, 50 hemodialysis patients were randomly assigned to the control and the experimental groups.
The inclusion criteria were as follows: being aged between 18 and 65 years, having last stage kidney failure that necessitates regular hemodialysis, having at least a six months’ history of hemodialysis, undergoing hemodialysis 1 to 3 times a week with each session lasting 3 to 4 hours, not having any intention of moving out of Jahrom or having a kidney transplant in the duration of the study, not receiving any organized education related to hemodialysis, not being affected by any psychological disorders, speaking Farsi, being literate, and owning a cell phone.
The exclusion criteria were: having experienced a traumatic incident during the 6 months prior to the study, taking anti-depressive drugs, hospitalization as a result of a serious disease, and unwillingness to participate in the study any further.
Data Collection
The quality of life of the subjects in both groups was evaluated using Ferrans& Powers Quality of Life Index Dialysis Version before and after the intervention. The patients in the experimental group were told not to share their education with other patients. Also, the researchers ascertained that the patients in the control group had not received any information.
The Questionnaire
1-In order to identify the patients’ needs, the researchers used a hemodialysis patients’ needs checklist. The checklist was taken from www.lifeoptions.org which is a comprehensive site designed by The Medical Education Institute in 1993 to help and educate patients with chronic kidney failures. The checklist, designed to help nurses identify their patients’ educational needs, is a researcher-completed instrument. The checklist addresses patients’ needs in 7 categories: medical issues, diet, relationship with family and friends, responsibility for treatment of one’s disease, future, lifestyle and daily activities, and relationship with medical staff (Poorgholami, BadiyepeymaieJahromi, Zamani, &KargarJahromi, 2016).
The content validity method was used to determine the validity of the checklist: the original quality of life scale was translated into Farsi and compared with the norms of the target populations; for standardization, the researchers consulted 10 experts in the field under study and used their comments to make the necessary revisions. Most of the items in the instrument in question were compatible with the culture and characteristics of our society. To determine the reliability of the instrument, the researchers used the split-half method: the study instrument was distributed among 10 hemodialysis patients and then the correlation coefficient between the odd-numbered and even-numbered questions was examined using Pearson correlation test. Once the reliability of the instrument had been confirmed with a correlation coefficient of r=0.9, the researchers used the checklist with the other subjects. In their study, Poorgholami et al. used the same checklist (Poorgholami, BadiyepeymaieJahromi, Zamani, &KargarJahromi, 2016; Moattari, 2012).
2-Ferrans & Powers Quality of Life Index Dialysis Version: This questionnaire was developed in 1986 by Carol EstwingFerrans and Marjorie Powers, professors at Illinois College of Nursing, to measure quality of life with regard to satisfaction with life. The instrument measures quality of life in two parts: satisfaction and importance. Part one consists of items that evaluate patients’ satisfaction and part two includes items that evaluate the level of importance patients attach to certain issues. The items are scored based on a 6-point Likert scale: in part one, the options range from “completely satisfied” (6) to “completely dissatisfied” (1) and in part two they range from “not important at all” (1) to “very important” (6). Ferrans & Powers’ scale consists of 68 items; each part includes 34 items and the items in both parts are similar. The index addresses four domains of quality of life: health and functioning (14 items), social and economic domain (8 items), psychological/spiritual domain (7 items), and family (5 items).
Using Cronbach’s alpha, Ferrans & Powers reported the scientific validity of the instrument to be 0.9 and 0.93 in 1985 and 1992 respectively (Poorgholami, BadiyepeymaieJahromi, Zamani, &KargarJahromi, 2016; Moattari, 2012); also, the scientific validity of the instrument has been confirmed through content validity, and its scientific reliability has been reported to be r=0.9 based on the retest method (Poorgholami, BadiyepeymaieJahromi, Zamani, &KargarJahromi, 2016;). At the beginning of the study, the subjects in both groups were given the necessary instructions about how to complete the forms and questionnaires. Then, before the intervention, the patients were asked to complete the quality of life questionnaire.
Intervention
the researchers, after subjects had acquired the necessary permits and made arrangements with the authorities at the hemodialysis ward, submitted a questionnaire that contained the inclusion criteria to the patients in the ward. The patients who were qualified were informed about the objectives and method of the study and asked to participate. Once the experimental and control groups were formed, all the participants completed a demographic, a checklist of hemodialysis patients’ needs, and a quality of life questionnaire. Subsequently, the program based on the continuous care model was implemented for the experimental group, while the control group received only the routine care.
For ease of making arrangements for the group classes, avoiding interference with the patients’ weekly dialysis sessions, and considering the similarities between the patients’ needs, the subjects in the experimental group were divided into 4 sub-groups, with 6 to 7 patients in each. These four sub-groups were exposed to the intervention based on the continuous care model.
Continuous Care Model (content of education)
The continuous care model is composed of several stages which were implemented in the following order for the patients in the experimental group:
Stage one is introduction and making the patients sensitive to their diseases and problems. The objectives of this stage are to help patients identify their problems correctly, stimulate patients, and point out the importance of follow-up care. Accordingly, the researchers arranged a 15- to 30-minute meeting with the subjects and their families to introduce them to the program, stimulate them, clarify the expectations, and stress the importance of follow-up care and continuing their clinical contact with the researchers throughout the specified period.clearly, unless this stage is executed, the program will not be successful: if patients and their families are made aware of the importance of the program, they will hopefully adopt a model of proper hygiene behavior. The intervention in this stage of the model was implemented through sessions that included counseling, group discussions, lecturing and asking and answering questions (with an emphasis on identifying the patients’ and their families’ current and future problems and needs, sensitizing the patients, and stimulating the patients to cope with their problems). Subsequently, each patient was educated individually three times—before, during and after a dialysis session—in the environment of the study and in the presence of his/her family.The number of sessions correlated with each subject’s knowledge and awareness and the severity and frequency of his/her problems. The patients and their families were asked to attend 7 sessions. Considering the level of patience of the participants, the length of each session was set at 60 minutes. If a raised question was outside the researchers’ field of knowledge, the patient would be referred to a specialist. The introduction and sensitization stage was executed in the first 3 weeks of the entire 3 month-period dedicated to the implementation of the model.
The objectives of the continuous care model can be achieved only if the continuity of the program is maintained; without proper follow-up and attention, even the best programs will be forgotten or lose their efficacy. Thus, since the adopted model was called the “continuous” care model,the rest of the time of the study was dedicated to follow-up which included: the researchers’ regular and effective physical presence during this stage of the implementation of the model, face-to-face or telephone counseling on a weekly basis and based on the subjects’ clinical needs, completing the check lists with the purpose of identifying new clinical problems, attention to the dynamic nature of health and disease, beginning sensitization for new problems, and observing the implementation and quality of care. In the present study, the follow-up was performed weekly and for some patients at every dialysis session and group session. Once the existence or non-existence of the previous problems had been ascertained, the researchers would set out to find out if there were any new problems and take the necessary clinical and counseling measures if there were any.Though evaluation was the fourth and last stage of the model, it was taken into consideration in all the stages.
Data Analysis
Finally, after the demographics and quality of life questionnaires had been completed and collected, the researchers used the chi-square test to compare the two groups’ variables and used the paired t- and independent t-tests to compare the difference between the means of the groups’ scores in SPSS 20.
Result
In the duration of the study, from each group, 1 of the subjects was excluded due to death, 2 were excluded due to kidney transplant, and another 2 were excluded due to unwillingness to participate further. Chi-square and ANOVA tests showed that both groups are similar in socio demographic characteristics. Table 1 shows some socio-demographic characteristics of the patients. The mean of quality of life scores in hemodialysis patients before intervention in each of the two groups are shown in Table 3. Independent sample t-test showed that there were no significant differences between the two groups in all quality of life subtypes before intervention. But after the intervention there were Significant differences between the two groups in the quality of life subtypes questionnaire. Thequality of life aspectsof the intervention group were higher than the controls.(Table 4)
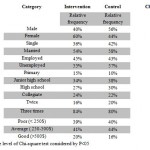 |
Table 1: Frequency distribution of the study units based on demographic variables in two groups |
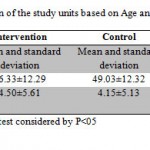 |
Table 2: Frequency distribution of the study units based on Age and Disease duration in two groups |
Note. Significance level of ANOVA test considered by P<05
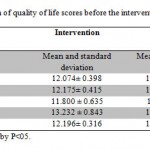 |
Table 3: Comparison of quality of life scores before the intervention in participant |
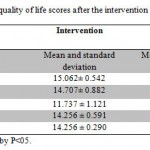 |
Table 4: Mean of quality of life scores after the intervention in the two groups |
Deterioration in quality of life is particularly evident inthe hemodialysis group of patients who have been on dialysis for an extended period of time. Most quality of life domains seem to be affected, including overall mental health. After taking into consideration that QoL deficits were mostly indicated by hemodialysis patients who had been on long term treatment, it could be argued that these patients experienced significant QoL changes over time, including deterioration in physical, social and environmental well-being as well as in overall mental health.( Simmons & Abress,1990).
Our results demonstrated that the QOL in intervention group increased significantly after the educational program. The total score and also aspects QOL scores were higher in the experimental group other than control group. By applying continues care model in the experimental group the QOL scores improved significantly compared to control.
Rahimi and colleagues found beneficial effect in their research on hemodialysis patients,( Rahimi, Ahmadi, &Gholya ,2006 )Ghavami and colleagues, in a study on diabetic patients,( Ghavami, Ahmadi, Entezami, & Memarian,2005) and other studies on elderly patients,( Salar, Ahmadi, & Faghihzadeh,2003) coronary bypass patients,( Sadeghi Shermeh,2009) and patients with chronic bronchitis(Salari, Mehdizadeh, Ebadi, Aslani, & Naderi,2009).
Since prevalence of patients undergoing hemodialysis, is high. It is necessary that we inhabit from load of cost of treatment and also increase process of recovery. For this issue suggested that to use educational program. Continues care model is considered to beeffective in increasing health related QOL inthese population (Hasanvandi,Valizade, Mehrabizade Honarmand, &Mohammadesmaeel, 2013; Hamid, 2011). Thus , providing such trainings can also be beneficial to hemodialysis patients.
Our results support the studies that showed a significant improvement on the quality of life outcomes in elderly people (Soo Oh, Kim, &SookSeo, 2005; Aging and Health, 2005).
Forouhari et al. did a study entitled “the Effects of training on quality of life in 62 menopause females”. The results showed a significant increase in the mean scores in all quality of life dimensions (Vasomotor, psychological – social, physical, and sexual) in intervention group (Forouhari, Safari Rad, & Moatari,2008).
The result of kate’ s study showed at 1 year, participants in the program experienced statistically significant improvements in health behaviors (exercise, cognitive symptom management, and communication with physicians), self-efficacy, and health status (fatigue, shortness of breath, pain, role function, depression, and health distress) and had fewer visits to the emergency department (Kate et al., 2001).
Considering chronic nature of the disease in patients undergoing hemodialysis, despair is inevitable in these patients. On the other hand, the role of this internal factor cannot be overlooked in self-care in these patients.
Conclusion
The present study results showed that continues training leads to increased QOL in the intervention group. Finally, this strategy can also be recommended for increasing QOL in patients suffering other chronic diseases.
Reference
- Ageing and health, a health promotion approach for developing countries, Available at: www.who.int.2005.
- Barone, C.P., Martin-Watson, A.L., &Barone, G.W.(2004). The postoperative care of the adult renal transplant recipient. MedsurgNurs. 13:296-302.
- Ebad, N., Sodani, M., Faghihi, A., &Hosseinpoor, M. (2009). The study of effectiveness of positive thinking training with emphasis on the signs of Quran on increasing hope to divorced women’s life of Ahvaz city. New Findings in Psychology, 4(10), 71-84.
- Forouhari, S., Safari Rad, M., &Moatari, M. (2008) Effect of education on quality of life in postmenopausal women referred to Motahari clinic in Shiraz. Journal of Birjand University of Medical Sciences 16.
- Georg, A.L., & Neilson, E.G.(2008). Disorders of the kidney and urinary tract. In: Fauci A S, et al, editors. Harrison’s principles of internal medicine. 17th ed. Mc Grow-Hill; p. 1726.
- Ghavami, H., Ahmadi,F., Entezami, H., &Memarian, R.(2005). The effect of applying of continuous care model in Diabetic patient quality of life. Uroumieh Med J. 16:22-7.
- Kate, R. L., David, S., Sobel, P., Ritter. L., Laurent, D., & Hobbs, M. (2001). Effect of a Self-Management Program on Patients with Chronic Disease. Effective Clinical Practice, November/December 2001
- KargarJahromi, M., Javadpour, S. H, Taheri, L., &Poorgholami, F. (2016). Effect of Nurse-Led Telephone Follow ups (Tele-Nursing) on Depression, Anxiety and Stress in Hemodialysis Patients. Global Journal of Health Science, 8(3), 168-173.
- KargarJahromi M. K, Poorgholami F, Rahmanian F, Rahmanian E. Effects of Self-Care Education with Telephone Follow-up on Self-Efficacy level in Hemodialysis Patients. BiosciBiotechnol Res Asia 2016;13(1)
- Hamid, N. (2011). Effects of Stress Management Training on Glycemic Control in Women with Type 2 Diabetes.Iranian Journal of Endocrinology and Metabolism, 13(4), 346-353.
- Hasanvandi, S., Valizade, M., MehrabizadeHonarmand, M., & Mohammadesmaeel, F. (2013). Effectivenessof 15591564.http://dx.doi.org/10.1016/j.sbspro.2013.06.788http://dx.doi.org/10.1016/j.sbspro.2013.06.788
- Moattari et al.: The effect of empowerment on the self-efficacy, quality of life and clinical and laboratory indicators of patients treated with hemodialysis: a randomized controlled trial. Health and Quality of Life Outcomes 2012 10:115http://dx.doi.org/10.1186/1477-7525-10-115
- NajafiMehri, S., Vahedparast, H., Hafezi, S., Saghafi, S., Farsi, Z., &Vahabi, S. (2008). Effect of selfcare
- Noohi, E., &Pouraboli, B. (2009). Educational Requirements of the discharged patients and their satisfaction
- Poorgholami F, Abdollahifard F, Zamani M, KargarJahromi M, BadiyepeymaJahromi Z. The Effect of Stress Management Training on Hope in Hemodialysis Patients. Global Journal of Health Science. 2016; 8(7).165-171
- Poorgholami F, Mansoori P, Montaseri Z, Najafi K. Effect of Self-Care Education with and without Telephone Follow-Up on the Level of Hope in Hemodialysis Patients; A Randomized Clinical Trial. IJCBNM. 2016;4(2):90-97.
- Sabetgadam M, Poorgholami F, BadiyepeymaieJahromi F, Parandavar F, Kalani N, Rahmanian E. Effect of Self-Care Education by Face-to-Face Method on the Quality of Life in Hemodialysis Patients. Global Journal of Health Science. 2016; 8(6):140-147.
- Poorgholami F, RahmanianKoshkaki A, KargarJahromi M, Parniyan R. A Study of the Influence of Group-Based Learning of Stress Management on Psychology Symptoms Levels of Hemodialysis Patients. Global Journal of Health Science. 2016; 8(11): 62-68.
- Poorgholami F, Javadpour SH, Saadatmand V, KargarJahromi M. Effectiveness of Self-Care Education on the Enhancement of the Self-Esteem of Patients Undergoing Hemodialysis. Global Journal of Health Science. 2016; 8(2): 132-136.
- Rahimi, A., Ahmadi, A., &Gholyaf, M.(2008). The Effects of continuous care model on depression, anxiety, and stress in patients on hemodialysis. NephrolNurs J. 35:39-44.
- Rahimi, A., Ahmadi, F., &Gholyaf, M.(2006). The effect of continuous care model in quality of life of hemodialysis patients. J Iran Med SciUniv; 13:123-32.
- Sabetghadam, M., Poorgholami, F., BadiyepeymaieJahromi, Z., Parandavar, N., Kalani, N., &Rahmanian, E. (2016). Effect of Self-Care Education by Face-to-Face Method on the Quality of Life in Hemodialysis Patients. Global Journal of Health Science, 8(7).
- SadeghiShermeh, M.(2009). The effect of applying of continuous care model in quality of life in patient after coronary artery bypass graft (CABG). Iran J Crit Care Nurs. 2:1-6.
- Salar, A., Ahmadi, F., &Faghihzadeh, S.(2003). The effect of continuous care model consulting in elderly people in Tehran. Zahedan J Res Med Sci. 5:261-7.
- Salari, M., Mehdizadeh, S., Ebadi, A., Aslani A, &Naderi, Z.(2009). The effect of applying of continuous care model in quality of life of chemical warfare victims with bronchiolitis obliterans. Kousar Med J. 14:101-7.
- Shu-fe, N., Chu, A.(2005). Quality of life of patient having renal replacement therapy. J Advance Nurs. 51:15-21.http://dx.doi.org/10.1111/j.1365-2648.2005.03455.x
- Sayin, A., Mutluay, R., &Sindel, S.(2007). Quality of Life in hemodialysis, peritoneal dialysis, and transplantation Patients. Transplant Proc; 39:3047-53.http://dx.doi.org/10.1016/j.transproceed.2007.09.030
- Simmons, R.G., Abress, L.(1990). Quality of life issues for end-stage renal disease patients. American Journal of Kidney Diseases 15:201-8.http://dx.doi.org/10.1016/S0272-6386(12)80763-3
- Soo Oh, H., Kim, M.K., &SookSeo, W. (2005). Effectiveness of behavioral Intervention Program for Urinary Incontinence in Community Setting. TaehanKanhoHakhoe Chi 35: 1476-1484.

This work is licensed under a Creative Commons Attribution 4.0 International License.



